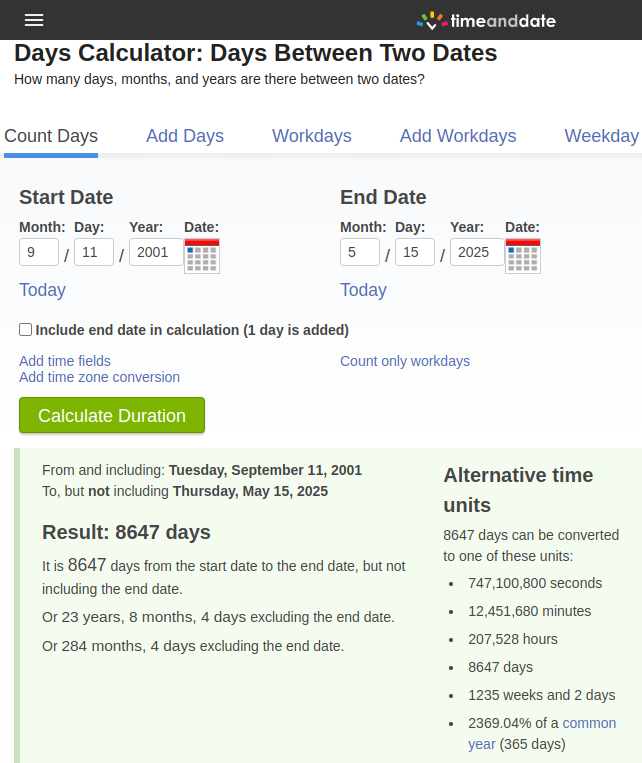
Cool shell formation on my beach walk - James Comey

By now I'm sure you've heard that former FBI director James Comey found a "Cool shell formation" on his beach walk -- and couldn't wait to post it on Instagram.

I'm also sure that you know what it means to "86" someone, and that Trump is the 47th president of the United States of America, -- and Comey's former employer.
There is one thing that is rather odd though. Someone pointed this out.
So, what does it all mean?
It means that James Comey would like for Trump to "go away."
What is the significance of 8,647 days from 9/11/2001? Comey might be a lot of things, but stupid isn't one of them. The date that the Instagram post was made is significant only in that it can provide cover, should any criminal charges be brought.
Because of these "coincidences" it would be very hard to prove any kind of "intent."
I predict that nothing is going to happen to James Comey, and that this was really more of a stunt to distract from the more important news -- that Trump has been making pro-America progress the Middle East.
What do you think?
Please leave a comment, like it or hate it... You DO NOT need to register to leave a comment. Email addresses are NOT used. Just make one up "someone@somehost.com"
There's Only One Thing The American Left Hates More Than MAGA
I recently came across this Axios article, and it exemplifies what's wrong with the American left.
The article is comprised of bullet points. Each point carefully worded to make anyone who supports Trump some kind of woman hating, racist Christian patriarch.
The article is titled, "Inside MAGA's fight for "Western civilization."
- The MAGA movement is no longer just fighting for President Trump. His most fervent loyalists are now engaged in what they see as a battle for "Western civilization" — a rallying cry for the modern right.
- For MAGA loyalists taking this long view, "Preserving Western Civilization" is the new "Make America Great Again."
- They proclaim America as a Judeo-Christian country that's the successor to the great European civilizations of Greece, Rome and the United Kingdom. They see a modern "Western civilization" as one that prizes freedom, the rule of law as they interpret it, meritocracy and the nuclear family.
- Trump policy attacks on asylum-seeking immigrants, and on programs benefiting historically marginalized communities, help reinforce that image.
- The period of U.S. history the movement heralds included subjugation of women, segregation, and discrimination against non-Whites, those in the LGBTQ community and many others.
- The growing pro-natalism movement encourages conservatives to have large families. Articles in far-right media tout marriage and children, and even advice for women on ways to be more "marriageable."
- In recent years, conservative activists have blasted college English departments for adding courses that focus on racially diverse writers, instead of staying focused on Shakespeare and Chaucer.
The author focuses on a few things in particular, but the list is rather innocuous. It's only when you combine all of the points in the list, including those that literally nobody is advocating for, that someone might think there's an issue. The article is written as a list of American leftist grievances.
I won't waste your time running through each point. Just a few are worth noting.
People who long for the 1950s are doing so, because it was a time of prosperity. You could support a family on a single income -- without a 4-year college degree. People were able to purchase a house, and start a family at a much younger age. These are the things that people want to see.
Large families are not a bad thing. Muslims often have much larger families than native-born Americans, nobody on the American left is complaining about large Muslim families.
There's nothing wrong with Christianity. Aren't we supposed to have freedom of religion?
Those who were championed by the American left, such as Bill and Hillary Clinton have made the same points Trump has made as it relates to immigration and deportations.
There is literally nobody calling for the discrimination of non-Whites.
The simple question is this, "How much of American Society would the author be OK with keeping?" This is an important question indeed -- because to change the country based on the above listed grievances, would result in an America that most people would not recognize -- nor would they want to live in.
On to The Second World!
el gato malo on Substack has done a spectacular post on the second world. Not many people understand this concept. It was more popular during the time of the Cold War.
if a society of low trust people adopts rules designed for high trust societies, it simply fails. none of the systems can function or establish themselves. it is only by first becoming high trust people that these sorts of structures may find foundation. the direction has to go that way.
so where then does “the second world” lie if not on the path from third world to first world?
i would posit that second world exists as a post 1st world stage and that you basically cannot get there without first having been first world. it’s not a transitional stage so much as a form of post achievement decline, a sort of senescence and degradation, a once lush garden gone to weeds. the second world is a trap and a truly nasty one from which extrication once caught is very difficult because the second world is, in many ways, the worst of all worlds, it’s first world systems that have fallen into hands and practices under which they cannot function, technology, technocracy, welfare systems, and systems of trust that work (or at least that can be managed at tolerable costs) by a certain sort of society but that become ruinous albatrosses around the necks of everything and everyone once they fall into disfunction, disrepair, and abuse.
This is true, placing people from low-trust societies into high-trust societies will not work. High-trust systems are not designed to deal with large amounts of people (trying to screw over other people) or perhaps just trying to survive in a system that they can't relate to.
Assimilation into a high-trust society is essential if the society is going to continue to function.
Read the bottom part first:
Otherwise you go from this:

To this:

And it can happen much faster than people might imagine.
Yuri Bezmenov on Substack did a brilliant article about a documentary that covers the struggles of two men Yang and Eddy, Yang's interpreter. The pair are working for the China Railway Engineering Company (CREC), in an attempt to build a road -- not a railroad, but a road for trucks.
Lao Yang is the modern day based Confucius - here are some of his greatest hits:
“You were governed by a European country for so long. You should have learned how things work…. Experience should be passed on. Only that way can you develop. You went backwards instead of forwards.”
“Look at your railways. High technology from the 1930s. We didn’t have it in China back then... You neglected the things others had left you. What’s more, you completely destroyed them. It will take generations to put things right.”
“They first constructed this road in 1954. More than 50 years ago. Since the Belgians built it you guys did nothing to maintain it…. Unbelievable. You can’t imagine the effort it took to built it. The infrastructure has gone to waste. It hurts to see it.”
“With regards to money we Chinese differ from the Congolese, who learned from the Belgians. Money or not, they spend it. No stress... On pay day the men go crazy. Two days later they come asking to loan them money. They don’t hold their drink that well. They just like drinking. They stand at the bar drinking beer. And then start shaking their behinds. It’s wonderful.”
“The government here isn’t efficient. We’ve been negotiating with them since the New Year. Half a year of talking without any results."
“People here don’t have any sense of time. It’s hard to adapt to life here. They waste time in almost everything they do. So we go back and forth.”
“I feel sorry for them. But sometimes I also hate them. Especially the thieves. They steal fuel and act all innocent.”
People from a high-trust society struggle to operate in a low-trust society, like Congo. People just steal the fuel, and go about their lives as normal.
"After all, if you wanted that fuel, why didn't you lock it up? And what made you think you could trust me with it anyway?"
Yang is operating in The Second World. Congo, a country that was rather developed, at least up until its independence in 1960.
The Second World is Already in The US
Consider California, once the downfall starts, it accelerates quickly from there. Once it has been determined that voting, or other peaceful means to slow or reverse the downward spiral (into The Second World) have failed -- people with the means to leave will do so.
California -- long ago -- decided to prioritize people -- other than its citizens. The tax-payers were put to the back of the line. You can only keep people hypnotized for so long, before they snap out of it, and realize that the walls are closing in on them. California is a failed state. As lawlessness increases, people leave.
It's not likely that things will turn around there in California in just one generation. Once the degradation starts, it accelerates, and attracts those who will accept those living conditions.
San Francisco:

Would you have believed that San Francisco would look like this in 2024?
Remember the movie "Back to The Future?" We were supposed to have flying cars by 2015, instead in 2024, we have giant homeless encampments -- because of "progress."

Granted they have moved a lot of the homeless off the streets very recently, but that was at a cost of 24-billion dollars. Keep in mind that these people are living in one of the most expensive places in the entire country. The median home price in San Francisco is 1.4 million dollars.
No matter what is done to "provide for the homeless," the situation is not sustainable. Getting homeless people off the street by paying for them is not a solution, it's only going to attract more people who are comfortable with that lifestyle.
Does Race Play A Role
Aly Dee on Substack did a very eye-opening post recently "Growing Up Anti-White."
She goes on to cover a range of issues, but these I found rather profound.
White Americans, for the most part, do not understand this because they do not believe similarly that other ethnic groups are the reasons for their failures. People speculate this is the case online, that there are many downtrodden White nationalists blaming blacks and browns for their struggles; however, your average White person is not terminally online on X (formerly Twitter) and still believes in a colorblind meritocracy.
What Whites do not understand about blacks and browns is our lore. I will not at all suggest that mainstream media hasn’t had its hand in brainwashing the ethnic masses; it has, but with our televisions off, we have a paradigm of the world that we are the underdogs. I speak from memory, so forgive me for some inconsistencies when going back and forth between past and present. I no longer believe the things I am describing to you, but as a young girl, I did to fit into my culture or because I took what my parents and educators said as gospel.
...
Subtly through the years, I was told by the adults around me that they weren’t successful because they were being discriminated against for being Black or Latin at their jobs. I thought, “Oh, well, that must mean the same thing is happening to me at school because I am Latina.” Never mind that I had gotten into the college I applied to and had a full-ride scholarship.This is why I say White Americans give Black and Brown Americans too much credit by blaming neomarxism for their ideology, it’s not like that. It’s this simple:
Ethnic minorities with a lower intelligence and/or an external locus of control blame White Americans for everything wrong with their lives, and the ethnic and White people around them corroborate this.
How do different races of people view each other? This is critical to understand what we're seeing in this country right now.
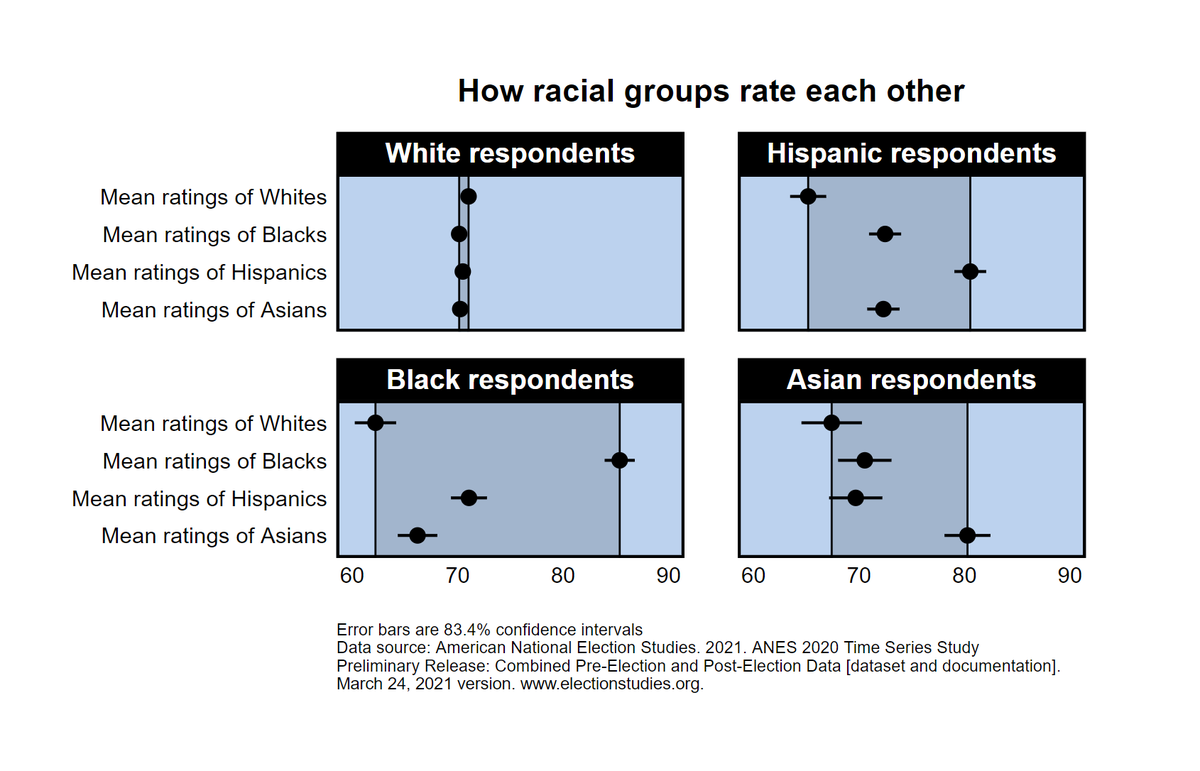
Perhaps this can bring a bit of understanding as to how things have progressed so far.
In all groups people have a more positive response to their own race, this is not a bad thing. In fact, in low-trust societies, it might just save your life.
Many people from low-trust societies can’t afford to look at people as "individuals" because the risk is too great. They necessarily profile, or be taken advantage of, robbed, or possibly killed. You don't want to trust the wrong person(s). In a low-trust society, a collectivist attitude is acceptable -- in fact it's expected.
A Twofold Problem
The people being brought here, are not coming here because they want to assimilate -- they're being brought here -- because they will not assimilate. Why might you ask? Consider which group of people is easier to control. American citizens -- who know their rights, or people from countries with drastically different legal and societal norms?
Consider all the people who have decided to self deport. They are doing this for one simple reason -- the Trump administration is upholding -- existing law -- and cutting off free benefits.
- As the article from Aly Dee makes abundantly clear. A large percent of the people being brought here -- by NGOs and the Biden administration -- feel as if the problems in their home country are the fault of White people -- the world over.
White American leftists in the US have added fuel to the fire, by constantly screaming "racism" at every turn. White people, or those who are considered White, are getting fed up with it, and that's why the whole attempt to pile on the Shiloh Hendrix ordeal failed miserably. People are tired of being told they're racist by people who illogically blame all their problems on White people.
Bringing people into the US who do not wish to assimilate, and who blame the indigenous population for their shortcomings, is obviously not a good idea. Most Americans are concerned with those who skip the line, and come here illegally, and still receive benefits -- for years -- leaching off the American tax-payer. All this, as the country goes deeper and deeper into debt.
People who come here on their own -- because they agree with American values, and respect the legal system -- and enter legally, is another story, but that's not what anyone is concerned with.
The American left portrays every Trump voter as looking for, a literal return to Rome.

This is a simple trick, an attempt to mischaracterize the serious concerns of American citizens who see the country that their relatives and ancestors fought and died for, being dismantled.
There is literally nothing that the American left is proposing that will benefit American citizens. This has never been more evident than it is now. American leftists flew to a foreign nation in an attempt to bring back a deported wife beating gang member, who was ordered to be deported twice already -- so he could be brought back the US -- then deported to somewhere other than El Salvador. More "progress."
Meanwhile, when American citizens were in need of help due to natural disasters, the American left was nowhere to be seen. And in fact, there was one person within FEMA that was denying help to people with Trump signs in their yard.
The Goal of American Leftists
The American Left cares not for the average US citizen. You are not them, and they do not want to try to convince you of anything. They want to rule, and they want free reign to implement their will upon others. It’s that simple.
The American left is through trying to convince you, trying to persuade you into seeing things “their way.”
The American left has realized that the American people are too smart to fall for the same tricks. They have pushed too hard, and shown their hand early. Now that their mask has come off -- the American people are rejecting the American left's plans entirely.
They have realized that people can’t be convinced to live in 15-Minute-Cities, in an Amazon box-sized apartment, with walls that all resemble an IKEA chest of drawers -- which more closely resemble a giant tackle-box.
If the American left has their way, they would gladly rule over an empire of dust. American leftists don't want citizens, they want serfs.
The only thing the American left hates more than Trump supporters, is American citizens.
What do you think?
Please leave a comment, like it or hate it... You DO NOT need to register to leave a comment. Email addresses are NOT used. Just make one up "someone@somehost.com"
Shiloh Hendrix “Straight Outta Compton” Rush Limbaugh and What Really Matters

By now, everyone has heard about the whole Shiloh Hendrix N-word fiasco.
The issue is not that Shiloh Hendrix used the N-word.
What those who claim to be offended truly care about is the fact that the N-word -- gives them power. The N-word is not offensive, because to those who claim to be victimized by it, gain massive power when it's used. They get an excuse to do whatever they want in its presence.
The reality is that it's just a word. Sure it might hurt some people's feelings, but then so might calling someone any racial slur.
It's not that there is really a major divide, it's that without the perception of a major divide, certain people lose their power. That power is illegitimate, and those who wield it instinctively know this -- that's why there's a constant drumbeat through media, music, and movies, to remind people of how divided we are. It's why people, both white and black, are not allowed to question the N-word in any way. It must not be discussed.
Does anyone remember the movie "The Village?" There were monsters that lived just outside the village in the woods, "Those We Don't Speak Of."

You cannot speak The Word We Don't Speak Of, because to do so, could potentially result in a logical discussion, and that's not allowed. To remove a word from use -- for a specific group of people -- is quite literally to stop all discussion.
Discussion, and realization are the enemy of such arguments, those arguments might be exposed as illegitimate. Keep that in mind, this applies to anything that people want to stop you from talking about.
The Word We Don't Speak Of is a form of social engineering and subversion -- designed specifically to cow people into submission. Although, not everyone accepts this programming, as we saw with Shiloh Hendrix.
There are many on both sides of the argument who disavow this plan to sow racial division. Consider this episode from the Rush Limbaugh show from 2016.
This particular episode does not deal with "The Word We Don't Speak Of" specifically, but it gets to the heart of the issue. The fact that the racial divisions in this country -- are driven -- by those who benefit from them.
A Young Black Man’s Brilliant Insights Inspired by Straight Outta Compton
Jul 29, 2016
RUSH: This is Curtis. Curtis is from Boca Raton. We had him yesterday. He was the last caller and we didn’t have enough time for him. He’s a young African-American. He saw Straight Outta Compton and he’s not comfortable with what he’s seeing here regarding all the rhetoric about cop killing and so forth and I think rap music. I think that’s what it was he wanted to talk about. We didn’t have time so I asked if we could call him back and he said yes. Curtis, thank you for letting us call you back. In your own words, what was it you wanted to say yesterday?
CALLER: Thank you for taking my call, Rush, I really appreciate it. Honored to speak with you. I got one main point, Rush, as a culture — and I’m black. I didn’t grow up with “African-American,” if you will. I’m just a black guy. As a culture, a people, I think we need to examine one of the main credos of gangsta rap music and its influence on the black community. Like I said, I saw Straight Outta Compton the other night. One of the scenes really touched me — and I’ll be really quick.
The rappers had signed a deal with a manager, they’re sitting on the stoop out on the street and eating lunch just innocently, two cops came up, overtly racist, overtly abusive. It was obvious. They made ’em get face down on the ground. Long story short, they got up after their manager’s help, went back inside, Ice Cube, who everybody knows is a main, famous rapper, stared the guy down, stared the cops down. The cops are just cursing him and degrading him. Went inside, and he penned one of their famous song songs, NWA, F’ the police.
RUSH: Hm-hm.
CALLER: And in the scene it was, you know, at that point of the movie I didn’t watch even the rest of it, at that point of the movie I was like, okay, he handled it as a man, he took the high road. He had an outlet, a creative artistic outflow, that’s great, but one of the things in this music or in this culture that is killing black people and inner city people is the fact or this credo of street cred. Now, any rapper will tell you, any rapper worth their salt will tell you, I live what I do, I’m real with this, that’s the work.
RUSH: Right.
CALLER: I’m not just fronting.
RUSH: When they have been questioned about this, I remember all this, the group NWA, I remember back in the early days of this show when examining cop killing lyrics and so forth, we had debates on this program about to what degree, if any, do lyrics like that in pop music influence cultural behavior and there were some people: “Come on, you can’t say that because there’s too much of it. It would be constant anarchy if that stuff was that influential.” And it is not just that stuff. I mean, you have all kinds of reprobate behavior in every movie you look at these days and yet —
CALLER: Well, the difference, Rush, excuse me, the difference that I see — and I’ve heard that argument, but I never saw Denzel going out and saying after a violent movie, “That’s how I roll.” I never saw Laurence Fishburne or Don Cheadle get up and say, “Yeah, that’s right, I keep it real.” We have this thing and it perpetuates the poison that’s in the minds of our young people, and they’re just like the poisoned minds of, you know, foregone generations who thought, you know, they walked up to somebody and say, “Hey, boy, hey, you black Negro.”
RUSH: Yeah.
CALLER: And now it’s the opposite, black kids can get away with walking up to people — and I witnessed it as a kid, I’m black and white — I witnessed people walking up on the basketball court to white people saying, “What up, white boy.” Or you hear in the movies today, people talking about, “What kind of white stuff is this?” It’s a double standard. It’s the same evil, bitter racist hate that’s infecting our youth today, and if we don’t confront it culturally from within and from without, it’s no better than racism coming from white lips or white people. It’s the same poison, Rush.
RUSH: You’re profoundly correct about this. But let me ask you about it from the standpoint or the context of what I believe is a genuinely divided country. I think there are two countries now. On the side that you were just talking about, if you have a genuine sit down with them, you learn that with them it’s a chicken-or-egg thing.
They will not deny that they have that attitude about the cops, but they will tell you that they didn’t start it. That the cops’ behavior towards them is what started everything, particularly the cops’ behavior toward innocent neighborhood blacks and that that music is simply the result of the culture and the music is the art that expresses how they have been forced to live and what their life experiences are.
And so when you talk about solutions, you eventually get, okay, well, where does the ultimate blame lie, because whoever is really responsible has to acknowledge it and either apologize, pledge not to do it anymore, and with neither side admitting that they had anything to do with starting it, how does it get solved?
CALLER: Well, I think it gets solved the same way that slavery got solved, the same way racism from white people got solved. We confronted it. We said, “This isn’t right how you’re treating people. This isn’t right how you’re raising your kids and teaching them and perpetuating this stuff.” We have to look at ourselves and say, look, there’s a real choice. Yeah, slavery was disgusting. Yeah, some police are bad apples and they do abuse kids, that’s disgusting, we need to stop it and stomp it out. But there’s a real choice that’s at hand, Rush. Everybody has to make it. One can just succumb to all this hate and lead one’s life — you know, the Palestinians do the same thing.
RUSH: Yeah.
CALLER: The Israelis do the same thing. When they’re, you know, imbued with hatred and taught to hate Arabs for no reason, Arabs taught to hate Jews for no reason, we have to stop and make a choice. We can succumb to all this hate and lead one’s lives like a script of bitterness with low aspirations or with too many excuses. Or we can overcome, we can fight, we can claw, we can dig, we can prevent all this perpetuating hate.
RUSH: That’s the most intelligent answer to this I have ever heard in all the years that I’ve been talking about this.
CALLER: Thank you.
RUSH: And as I listened to you say it and I imagine it being implemented, the people that actually try to do that, I’m thinking, you know, you naturally think okay, what will some of the obstacles be? And one of them is that, for whatever else is going on, there are a lot of people who have gotten really rich, I mean, really wealthy as a result of this art form, hip-hop, rap, whatever you call it. And you’re gonna be asking some of them to basically throw away their vehicle to financial independence and wealth by asking them to get rid of that kind of lyric line in their art or in their music.
CALLER: I don’t know that it’s necessary to get rid of it. It is expressive just like a Mafia movie or an action movie, but I would challenge them and those listening, anyone who perpetuates that stuff. I would challenge them this way, Rush: “If you really care about black people, about inner city people, about the ghetto, about the ‘hood — if you really want solutions — then at least admit that though you might have ‘slung rock’ in the past, been a dope dealer, been a bad boy in the past, that’s fine.
RUSH: Well.
CALLER: “But listen, kids, we can’t continue this. This is just entertainment.” Because the kids aren’t hearing it. They emulate these guys because these guys portray the reality of it.
RUSH: Amen.
CALLER: And, you know what? All the other charlatans who’ve gotten rich, too, if they really care, let’s get down to Chicago. Let’s hold arm in arms with the soldiers that are marching in the streets and helping — trying to help — the community bridge the gap with gangs and all that stuff. If these rich artists and rappers really care, which I believe some of them really do, then let’s get back to the community in a real way instead of this.
RUSH: That inspires another question. How many…? I guess we don’t know, but how many of them really want a solution to it? I can… You know, my understanding (some would say “fear”) is that there are a lot of people — not rappers, but I’m talking about race-business executives — making a lot of money on the basis that this strife and conflict is never ending.
CALLER: Because they keep the cycle of victim going, Rush.
RUSH: Right.
CALLER: And that’s —
RUSH: So if some of these people don’t want a solution… I’m sorry to keep throwing up obstacles to you, but the reason I am is because you’re really… You’ve got brilliant answers here. I’m imagining I’m not going to be able to stump you on anything.
CALLER: I think most black people, white people, all people, Americans, we need to stand up and say, “Listen, Jesse Jackson, listen Al Sharpton, listen race-baiters, whoever you may be — of whatever political stripe you may be, I don’t care — if you’re gaming the system and if you’re perpetuating hate in our kids’ hearts, I don’t care if you’re a rapper, you’re a politician, you’re an Action Coalition, you’re a street organizer. Whatever you call yourself, if you’re perpetuating this in our children’s hearts, stop.
“Because if you don’t stop, it’s just showing them that they can be bitter, they can be bigots, they can call people ‘white boy.’ They can be racist, and because they’re black…” And enough of this stuff, too, Rush, with the, you know, “Black people can’t be racist.” That’s baloney. And they say they can’t be racist because they have no power? So how can Little Johnny White Boy be a racist if he has no power? It’s a sham, Rush.
RUSH: Yeah. It is.
CALLER: And I’m tired of it. I’m sick of it. It pains my heart for black people, for America —
RUSH: It does mine, too.
CALLER: — for kids who are really struggling.
RUSH: It pains —
CALLER: Exactly.
RUSH: Nobody wants an America like that. Well, I say “nobody.” Most people, it pains their hearts. It certainly does mine. Every one of those cop shots, every… The whole Ferguson thing, the fact that it happened, the way it went down? Nobody wants this.
CALLER: That’s right.
RUSH: It seems so senseless. Can you hang on through the break? I’ve gotta take a break. There’s one other question I have for you.
CALLER: Yes, sir.
RUSH: Okay, good. You see why when we only had a couple minutes yesterday, my instincts said it was not enough time? So he let us call back again today.
BREAK TRANSCRIPT
RUSH: Back to Curtis in Boca Raton. I wanted to ask you a personal question. What do you do? And you don’t have to answer it if you don’t want to.
CALLER: I’m a manager at a Financial Services Company.
RUSH: And have you…? You’ve thought about this, obviously extensively. Have you —
CALLER: Yes, sir.
RUSH: Have you any aspirations to do anything to actually help implement some of this? Do you have political aspirations?
CALLER: Yeah, absolutely. Between the day job and, you know, just making a living, I just got married about eight weeks ago. Absolutely, Rush.
RUSH: Congratulations, by the way. (clapping)
CALLER: Thank you, sir.
RUSH: Happy to hear that for you. Well, we wish you the best here, and I really… It’s fortuitous that you got through here yesterday; it’s fortuitous that you let us have your phone number to call you back when we didn’t have time. ‘Cause, Curtis, I’m telling you honestly: You had some of the most insightful and intelligent answers to this that I have ever heard, primarily and spectacularly your answer when I asked, “How do you deal with the fact that for some of these people, that’s their reality?”
It’s a chicken-and-egg thing. Look, who started it? There is a definite thing to blame and if they won’t blame it, your answer was we just have to face it head-on like we faced slavery. Anyway, it was interesting because it highlights all the obstacles that are in the way. And one of the obstacles is personal wealth. There are a lot of people… This not a criticism; it’s an observation. It’s kind of important here. There are a lot of people who have gotten incredibly wealthy with these lyrics and that art form.
And there are other people getting incredibly wealthy claiming to have some sort of solution to this strife, but in truth don’t want any solutions because the strife and the conflict is how they have become known. So it’s a… But it is ripping the country apart. It’s also… By the way, Curtis, it also has political sponsorship. That’s another thing. We didn’t even get into that aspect of it. But when you ask who benefits from all this, there are certain people in a certain political party who’ve made sure they benefit from it. But I hope that people with ideas like yours ultimately prevail.
What do you think?
Please leave a comment, like it or hate it... You DO NOT need to register to leave a comment. Email addresses are NOT used. Just make one up "someone@somehost.com"
The Magic of Crowds and Power
For this post, I’m going to quote an entire article. I don’t often do this, but this article is exquisite in it’s detail, and capturing of the emotion, and logic (or sometimes lack thereof) of the “Obama Movement.”
There is something odd -- and dare I say novel -- in American politics about the crowds that have been greeting Barack Obama on his campaign trail. Hitherto, crowds have not been a prominent feature of American politics. We associate them with the temper of Third World societies. We think of places like Argentina and Egypt and Iran, of multitudes brought together by their zeal for a Peron or a Nasser or a Khomeini. In these kinds of societies, the crowd comes forth to affirm its faith in a redeemer: a man who would set the world right.
As the late Nobel laureate Elias Canetti observes in his great book, "Crowds and Power" (first published in 1960), the crowd is based on an illusion of equality: Its quest is for that moment when "distinctions are thrown off and all become equal. It is for the sake of this blessed moment, when no one is greater or better than another, that people become a crowd." These crowds, in the tens of thousands, who have been turning out for the Democratic standard-bearer in St. Louis and Denver and Portland, are a measure of American distress.
On the face of it, there is nothing overwhelmingly stirring about Sen. Obama. There is a cerebral quality to him, and an air of detachment. He has eloquence, but within bounds. After nearly two years on the trail, the audience can pretty much anticipate and recite his lines. The political genius of the man is that he is a blank slate. The devotees can project onto him what they wish. The coalition that has propelled his quest -- African-Americans and affluent white liberals -- has no economic coherence. But for the moment, there is the illusion of a common undertaking -- Canetti's feeling of equality within the crowd. The day after, the crowd will of course discover its own fissures. The affluent will have to pay for the programs promised the poor. The redistribution agenda that runs through Mr. Obama's vision is anathema to the Silicon Valley entrepreneurs and the hedge-fund managers now smitten with him. Their ethos is one of competition and the justice of the rewards that come with risk and effort. All this is shelved, as the devotees sustain the candidacy of a man whose public career has been a steady advocacy of reining in the market and organizing those who believe in entitlement and redistribution.
A creature of universities and churches and nonprofit institutions, the Illinois senator, with the blessing and acquiescence of his upscale supporters, has glided past these hard distinctions. On the face of it, it must be surmised that his affluent devotees are ready to foot the bill for the new order, or are convinced that after victory the old ways will endure, and that Mr. Obama will govern from the center. Ambiguity has been a powerful weapon of this gifted candidate: He has been different things to different people, and he was under no obligation to tell this coalition of a thousand discontents, and a thousand visions, the details of his political programs: redistribution for the poor, postracial absolution and "modernity" for the upper end of the scale.
It was no accident that the white working class was the last segment of the population to sign up for the Obama journey. Their hesitancy was not about race. They were men and women of practicality; they distrusted oratory, they could see through the falseness of the solidarity offered by this campaign. They did not have much, but believed in the legitimacy of what little they had acquired. They valued work and its rewards. They knew and heard of staggering wealth made by the Masters of the Universe, but held onto their faith in the outcomes that economic life decreed. The economic hurricane that struck America some weeks ago shook them to the core. They now seek protection, the shelter of the state, and the promise of social repair. The bonuses of the wizards who ran the great corporate entities had not bothered them. It was the spectacle of the work of the wizards melting before our eyes that unsettled them.
Daniel Patrick Moynihan, the late Democratic senator from New York, once set the difference between American capitalism and the older European version by observing that America was the party of liberty, whereas Europe was the party of equality. Just in the nick of time for the Obama candidacy, the American faith in liberty began to crack. The preachers of America's decline in the global pecking order had added to the panic. Our best days were behind us, the declinists prophesied. The sun was setting on our imperium, and rising in other lands.
A younger man, "cool" and collected, carrying within his own biography the strands of the world beyond America's shores, was put forth as a herald of the change upon us. The crowd would risk the experiment. There was grudge and a desire for retribution in the crowd to begin with. Akin to the passions that have shaped and driven highly polarized societies, this election has at its core a desire to settle the unfinished account of the presidential election eight years ago. George W. Bush's presidency remained, for his countless critics and detractors, a tale of usurpation. He had gotten what was not his due; more galling still, he had been bold and unabashed, and taken his time at the helm as an opportunity to assert an ambitious doctrine of American power abroad. He had waged a war of choice in Iraq.
This election is the rematch that John Kerry had not delivered on. In the fashion of the crowd that seeks and sees the justice of retribution, Mr. Obama's supporters have been willing to overlook his means. So a candidate pledged to good government and to ending the role of money in our political life opts out of public financing of presidential campaigns. What of it? The end justifies the means.
Save in times of national peril, Americans have been sober, really minimalist, in what they expected out of national elections, out of politics itself. The outcomes that mattered were decided in the push and pull of daily life, by the inventors and the entrepreneurs, and the captains of industry and finance. To be sure, there was a measure of willfulness in this national vision, for politics and wars guided the destiny of this republic. But that American sobriety and skepticism about politics -- and leaders -- set this republic apart from political cultures that saw redemption lurking around every corner.
My boyhood, and the Arab political culture I have been chronicling for well over three decades, are anchored in the Arab world. And the tragedy of Arab political culture has been the unending expectation of the crowd -- the street, we call it -- in the redeemer who will put an end to the decline, who will restore faded splendor and greatness. When I came into my own, in the late 1950s and '60s, those hopes were invested in the Egyptian Gamal Abdul Nasser. He faltered, and broke the hearts of generations of Arabs. But the faith in the Awaited One lives on, and it would forever circle the Arab world looking for the next redeemer.
America is a different land, for me exceptional in all the ways that matter. In recent days, those vast Obama crowds, though, have recalled for me the politics of charisma that wrecked Arab and Muslim societies. A leader does not have to say much, or be much. The crowd is left to its most powerful possession -- its imagination.
From Elias Canetti again: "But the crowd, as such, disintegrates. It has a presentiment of this and fears it. . . . Only the growth of the crowd prevents those who belong to it from creeping back under their private burdens."
The morning after the election, the disappointment will begin to settle upon the Obama crowd. Defeat -- by now unthinkable to the devotees -- will bring heartbreak. Victory will steadily deliver the sobering verdict that our troubles won't be solved by a leader's magic.

This way of thinking applies as much to Obama, as it does to Trump now.
People are looking for a savior – and they shouldn’t be. No politician is going to save anyone. That’s a very dangerous belief. It’s not a wise position to put oneself in.
Don’t project yourself onto other people, and imagine that their wishes are your wishes. It’s not realistic, and will nearly always lead to disappointment.
Do I think that Trump is going to do some good things (as it relates to the American citizens) yes. But I also think he’s going to put in place some measures that might prove very damaging in the future. Precedence is a dangerous thing. Sure it might be (set / used) to remove damaging policy right now, but it might also be used to instate damaging policy at a later time.
We’re witnessing a perfect storm of illegitimacy. None of the branches of government are actively doing what they are supposed to do.
The SCOTUS is ruling in ways that do not truly uphold The Constitution. (Obamacare / the ACA) was rewritten by Chief Justice Roberts – to make it legal. Why? It was bad law, everyone knew this. Anyone who looked at the mechanics of it knew that it was not Constitutional (Roberts proved this by rewriting parts of the legislation).
Repealing the ACA never happened. This was not by accident either. Why is Obamacare still law?
Why have most people stopped talking about it?
Why did Trump praise the COVID-19 vaccines during Biden’s State of The Union Address in 2024?
How is it that the war in Ukraine is the least-televised and least-broadcast in history? I remember watching the Gulf War on cable TV each night in the 1990s. They even made fun of it in movies at the time.
Video game footage was said to be real — and this was echoed by the Ukrainian Military.
CLAIM: Video shows the Ukrainian air force shooting down a Russian air force fighter jet in Kyiv.
AP’S ASSESSMENT: False. The footage is from the video game Digital Combat Simulator, according to the YouTube user who uploaded the clip on Feb. 24.
THE FACTS: Social media users on Thursday misrepresented footage from a video game showing close combat between two fighter jets, claiming the clip showed the Ukrainian air force shooting down a Russian fighter.
“Footage of a MiG-29 of the Ukrainian Air Force shooting down a Su-35 fighter jet of#Russia’s Air Force over Ukraine’s capital#Kyiv today,” reads one false tweet.
The Ministry of Defense of Ukraine’s official Twitter account also shared the clip with the false caption.
Now we have Starlink, 24/7 Internet, phones with cameras built-in, and yet there's very little known about what has really happened in Ukraine – outside of "officially approved” channels. Why is that? There was more known about Vietnam. But this modern war, not much of anything. Where are all the independent journalists? Where’s Geraldo Rivera to draw military movements in the sand? Doesn’t it all seem a little odd?
Things are not what they seem – know this.
What are the answers to all this? I don’t know. I just know that we’re being led down the primrose path from every angle.
Don’t succumb to this belief that everything is going to be OK. It’s likely not. Does that mean it’s the end. Of course not. Things always ebb and flow.
We (free thinking people) haven’t “won.” Things are just changing again. Navigating all of this will be insanely complicated, but simple things still work.
We’re now in a time of competing manipulations, or manipulative abilities. It’s a war of manipulation, because the people who truly want control know that they can’t do it without willing participants. Ever wonder how so few rule so many?
Convincing people doesn’t work fast enough. There’s history involved, it gets complicated, so people have to be corralled much more quickly now. Don’t give people time to think – force them into reaction.
Just as the Internet freed people, and allowed for the free flow of knowledge – knowledge that overcame the previous manipulation(s) – now the Internet is being used to limit knowledge – to further manipulations.
It’s not a new concept, it’s an old concept, it just has more reach, and can manipulate people on a mass scale – much more quickly than at any other point in time. Don’t let politicians (on either side) convince you that they believe in your ideas – because they don’t. The only people who might are people on the street – and they’re not likely to come to power anytime soon.
If I had any advice to give it would be this. Enjoy the good things, but notice the bad things (and most importantly how they came about). Don’t become stuck. Keep your eyes open – don’t become caught up in nonsense – because nonsense is going to come from all sides now, and it’s going to come fast and hard.
Don’t fall prey. Go outside and talk with your neighbors. Talk with the people at the grocery store.
What do you think?
Please leave a comment, like it or hate it... You DO NOT need to register to leave a comment. Email addresses are NOT used. Just make one up "someone@somehost.com"
Is The New Waste Collection Service Trash?
Where I live there is a new waste collection company. They require garbage to be picked up in bins like these.

They each hold 95 gallons. Of course, that’s if all of your garbage was liquid -- which it will never be.
We are a family of four, and I could only swing a single can if I took the other larger stuff that we throw away, and compress it, by drawing all the air out of the bag with a vacuum cleaner.
I have broken down boxes and larger stuff in 55 gallon bags from Sam’s Club. I was able to put them at the curb, filled with light stuff, and the other company would just toss them in the truck no questions asked. But we can't do that anymore.
Fitting all of that in one 95 gallon can was not working. I decided to spring for the extra can. It is $65 dollars a year to lease it, and $15 a quarter for collection.
Bottom line, it’s a pain in the neck. This change costs the taxpayer more money in the end, it’s just not collected in taxes -- it’s collected through the waste removal company. But I’m sure it looked good on paper. It saves the county money, just not the residents.
Anyway, because these garbage carts don’t close with any kind of seal, they can get quite nasty before the weekly pickup day, flies and whatnot.
I’ve seen many options to keep this from happening. One of the most interesting was taking a feminine napkin (maxi-pad) soaking it with Pine-Sol, and sticking it to the under part of the lid. While I’m sure this works, it seems like a real pain, because the pads will need replacing frequently. Also the cans that we have are black, and this is Florida, so they’re going to be extremely hot most of the time.
Another interesting option was this.

This was a great option, because it doesn’t require too much work. However, you’ll have to remove the laundry bag before collection. Because of the way the truck picks up the can, you’re likely to lose your laundry bag and bungee cord.
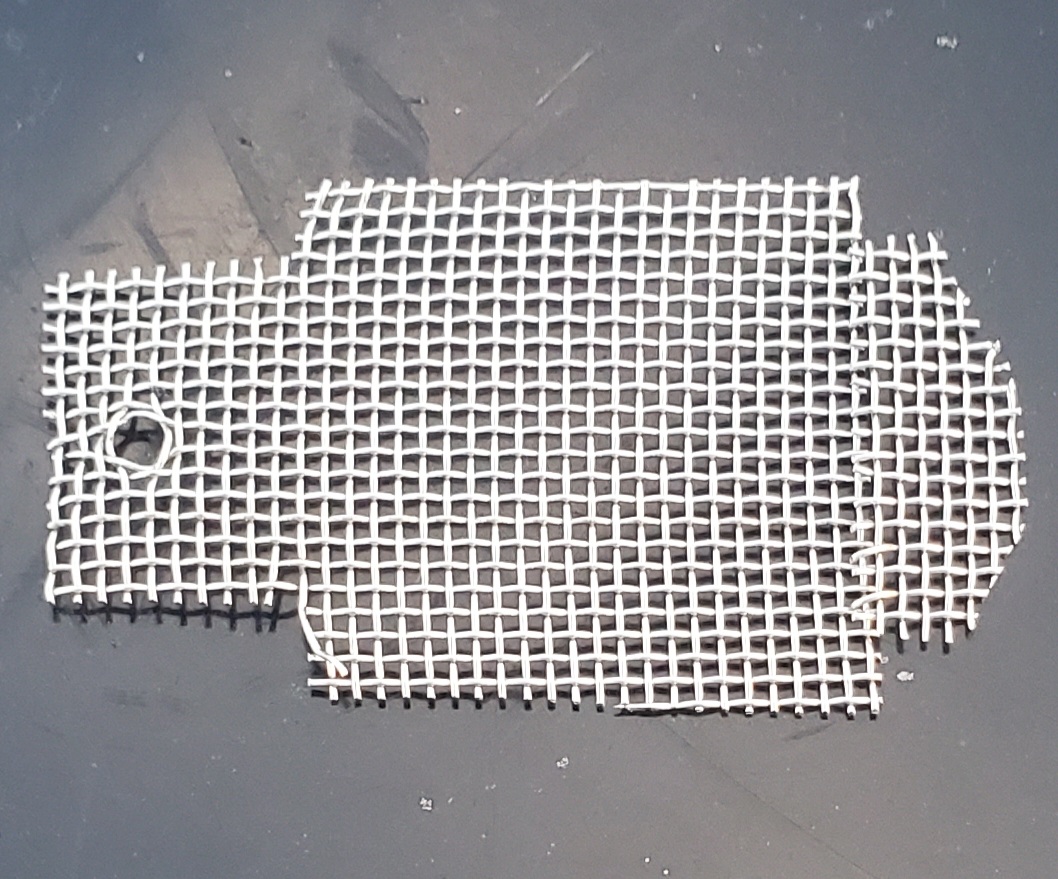
So, I came up with my own method, stainless steel screen. I know that most people don’t have this laying around -- but I do. I originally bought it to make sand sifters for shark’s teeth at the beach. They came in a pack of four 11” x 14” pieces. So, I had plenty left over to use for other stuff.
After looking at the can, there is only one place where flies can get in (with the lid closed). There are two vents at the back of the can. So, I decided to make screens to cover those openings.
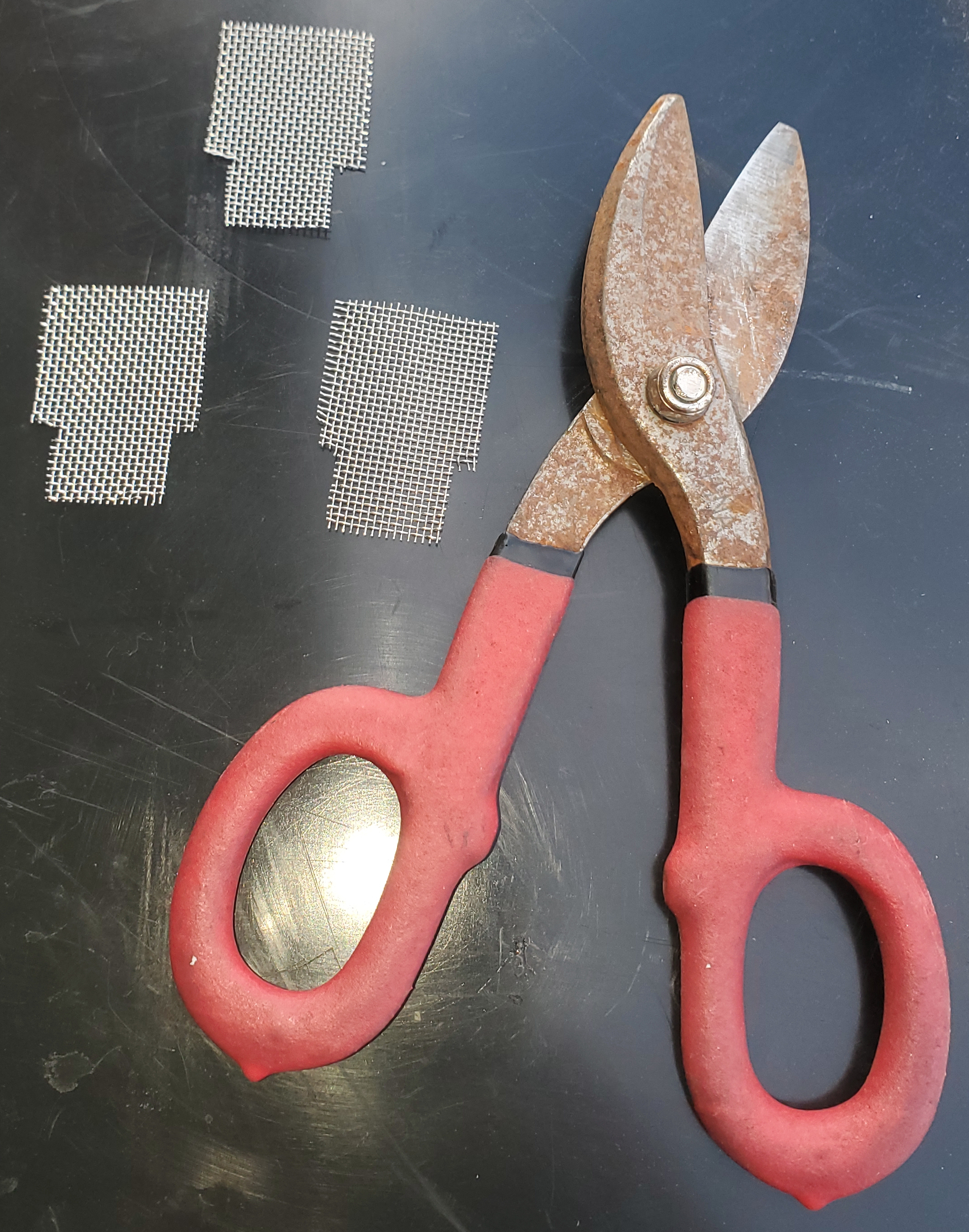
I secured them with "stingers" those little framing screws that are super sharp. That's why they call them stingers, because when you reach into the bag they sting you!

This appeared to be a great solution. No pieces to replace, easy to make and install, problem solved right?


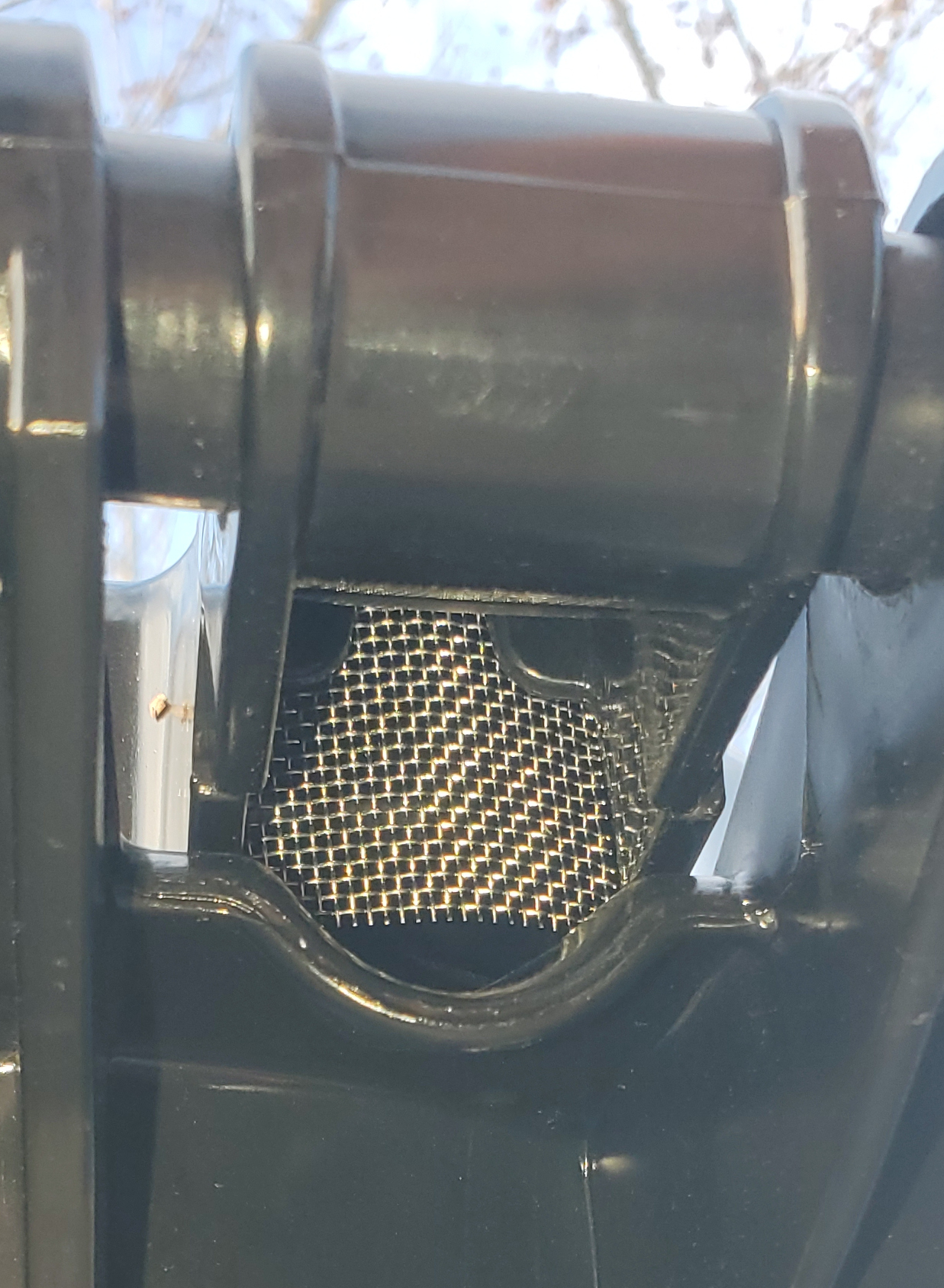
Well, not so simple it seems, I didn’t realize that the curved part was literally where the screens would sit down.
The screens needed to be modified. So I came up with this shape. I already installed them but they are shaped like this.
Here's what the openings look like now with the modified screens installed.


No flies are getting in now!
I now have a solution that doesn't require babysitting.
What do you think?
Please leave a comment, like it or hate it... You DO NOT need to register to leave a comment. Email addresses are NOT used. Just make one up "someone@somehost.com"