Conspiracy Theorist's Advocate (2)
Lets face it, things just aren't right.
Lately conspiracy theories have become working theories with astounding frequency. That's not a good thing.

Does infection-acquired immunity outperform vaccines?
The immunity generated from an infection was found to be “at least as high, if not higher” than that provided by two doses of an mRNA vaccine, the authors wrote.
While Murray and Wachter agreed that vaccination remains the safest route, having a past Covid infection should at least be considered in policymaking decisions going forward, such as vaccination requirements, they said.
“What Europe did with this evidence made a lot of sense, which is where evidence of past infection was seen as essentially equal to vaccination in terms of requirements to go into events or for employment,” Murray said.
At the very least, he added, officials should accept that evidence of recent infection is equivalent to vaccination.
Notably, the immunity acquired from infection did appear to wane more slowly than the immunity from two doses of an mRNA vaccine.
What does this mean? It means that all of those people who were singled out for not getting the COVID-19 vaccine because they already tested positive and recovered -- were right and should have been left alone. Think of all the people's lives that were turned upside down simply because they didn't follow a government dictate. There were families that were torn apart over the issue of vaccines. I personally took steps to insure that my wife would no longer have to work. In truth, the government response to COVID-19 was orders of magnitude worse than COVID-19 itself.
Not only that, because of the Twitter Files releases, we know that the government was working to suppress the information found in the article above -- for two years! The government was aware all along that natural infection was better than vaccination. But at every turn the government and its associated "public health officials" lied, and misrepresented data, to insure that the most people possible were vaccinated.

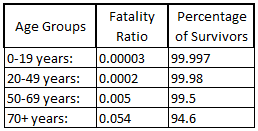
In order to get the percentages representative of the number of people who were infected and survived, just multiply the Infection Fatality Ratio by 100 to make it a percentage, then subtract the value from 100. You can do the math in a spreadsheet and you end up with:
= 100 - (Fatality Ratio*100)
This should not be forgotten. Our own government has done more to damage the US people in general and the economy than any foreign enemy could ever hope to do. The question is why?
Let's continue.
EAST PALESTINE, Ohio (WKBN) – The U.S. Environmental Protection Agency sent a letter to Norfolk Southern claiming it failed to properly dispose of contaminated soil after the train derailment in East Palestine.
According to the letter, “Five railcar tankers of vinyl chloride were intentionally breached; the vinyl chloride was diverted to an excavated trench and then burned off. Areas of contaminated soil and free liquids were observed and potentially covered and/or filled during reconstruction of the rail line including portions of the trench /burn pit that was used for the open burn off of vinyl chloride.”
“I think it was not in the best interest of human health and welfare and the environment to simply cover it up and keep going without at least a preliminary evaluation to determine if the level of vinyl chloride that was present in the soil was going to create a potential contamination threat to surface or groundwater,” said Dr. Julie Weatherington-Rice who has a Ph.D. in soil science and has been working for Bennett & Williams Environmental Consultants since 1986.
Why was Norfolk Southern just covering up toxic chemicals -- before the EPA was on the scene? I would think that this kind of action would lead to serious fines, if not put individuals with Norfolk Southern at serious legal liability. Executives at Norfolk Southern had to know that nothing of consequence would come from their actions. How they knew that, I'm unaware, but it's certain that there was little concern on the part of Norfolk Southern executives as it relates to burying toxic chemicals.
A former EPA official weighs in on the East Palestine accident on PBS.

MEIBURG: Well, there are a couple of things. One is I will be specifically watching for continued monitoring, not because I think there's going to be much new information from it, but it's important to do that to reassure people that, in fact, you're continuing to watch. Secondly, there'll be continued sampling, especially water sampling and groundwater sampling, to see if there is any long-term contamination in groundwater or soils around the site of the accident. So those are two things that I would watch for.
Considering the US government's recent track record, I can't ignore how badly things have gone. And it's not just these two incidents. There are many incidents that have occurred over the last few years, here are (7) that come to mind.
1. Tyrannical COVID-19 Mandates
2. Border Crisis / Open Border
3. Deadly Afghanistan Withdrawal
4. Energy Dependence
5. Crime Surging
6. Rising Inflation
7. War on Parents and Americans in general
All of the things I listed above have resulted from policy changes -- at the onset of the Biden regime. These are also all outcomes that were completely predictable.
It's not that government officials are incompetent -- but this might all be on purpose. Why would anyone want to feign incompetence? I believe I might have the answer.
Consider, if the majority of Americans lose faith in the federal government's ability to function, on nearly all levels, who are they going to blame? The media is going to try and pin most of this on Trump, the illogical nature of such accusations are irrelevant. The idea is to make it known to the general public that the US government's most important agencies have failed on multiple levels. The CDC failed with COVID-19, while the European nations did better under the direction of the WHO (World Health Organization). Couple all of this with the Biden regime handing over control of the US Public Health apparatus to the WHO, and you have a seriously strange situation.
Could it be that US government agencies will prove to be untrustworthy, and incompetent? I believe that's precisely the point of this exercise. The idea being that the US government's agencies need to be replaced by a much more "diverse global government" that's not corrupt and incompetent. Why else drive every US agency straight into the ground, while simultaneously dissolving US sovereignty through globalized health directives?
If you have a better argument, let me hear it.
Note: You DO NOT need to register to leave a comment. Email addresses are NOT used. Just make one up "someone@somehost.com"
The QR code below links to WindUpRubberFinger.com for easy sharing.
Military Strategy and Balloons
There are many strategies in war, but some work regardless of the opponent -- or their technological capabilities.

Years ago I read about how during the cold war Russian soldiers were trained to carry out missions nearly entirely based on time. I can’t find any of this information now because an Internet search will only bring up the Russia-Ukraine conflict.
The reason Russia went with this type of strategy was simple. Both the US and Russia could monitor radio frequencies and intercept communications, otherwise making ground forces vulnerable. The US, long ago, had the ability to decrypt digital encrypted communications in almost real time. Also, any transmissions sent would be scrutinized. Those transmissions, even if not decoded, could still be recognized and used for a counteroffensive. This meant that there was no “safe” way to communicate with ground forces once they were in the field. So, timing was determined to be the best way.
Russian soldiers were to go out, and perform various parts of their mission at precise time windows, to avoid the need for communications. This was a rather brilliant plan. Of course, a lot could go wrong, but a lot could go right. Also, there was little chance that the opponent would know what you’re planning, because everything just “happens.” This puts the opponent on a reactive footing for nearly the entire operation.
This brings us to the balloon issue. We know that the first balloon that made it into the news was rather large, and had a huge array of instruments suspended from it. Whatever it was sent here to do, it was not disguised, and there was no attempt to hide it. So, why was it here?
The answer to that question would require honest military leaders, which we are sadly short on these days. There are a few different hypotheses for this event. I will list a few possibilities that I have considered.
After reading a rather interesting Substack post, the payload came into question. Of course the last balloon that was shot down had “strings hanging from it” according to one of the F-16 pilots. The writer pointed out that during the Vietnam war, the US put seismic sensors all along the Ho Chi Minh trail. This alerted the US military as to when the Viet Cong were moving supplies by truck, and could send in an air strike to maximize their effectiveness. These devices were not transmitting unless there was enough seismic activity, so they were largely undetectable. So, where did the balloon's payload go?
CBS ran a story on this very issue, apparently nobody knows.
“Assistant Secretary of Defense Melissa Dalton said in a briefing with reporters on Sunday that the U.S. has been more closely scrutinizing airspace at certain altitudes, including enhancing the radar.
“The unidentified object that was downed near Alaska was the size of a small car, according to the Pentagon. The object shot down over Lake Huron appeared to be octagonal in shape with strings hanging off, but no discernible payload, a senior administration official said.”

The first balloon was very obvious, the balloons that followed were much smaller and harder to detect. But they were able to make it over US territory. Why? Well there are a few reasons for that. Active surveillance is the reason that most people are stating. It was said that the US military made sure the first balloon wasn’t transmitting data. Which really means, it wasn’t transmitting data. So, what was it doing.
I have a few theories on this. Let’s incorporate the payload, and time aspect into this. Let’s assume that China is going to invade Taiwan, everyone thinks that this is going to happen at some point. The question is when? Now how could these balloons help the Chinese war effort? The balloons can deploy small units on the ground (their payloads). These units that can determine what’s going on around US military installations, or anywhere else that they drifted over.
These units don’t need to broadcast continually, perhaps only once initially. They can send one broadcast to transmit their relative location (using US GPS coordinates) then wait. China knows when it’s going to invade Taiwan, they can have these units sleep until they begin military operations. Using this method, the devices will remain undetectable because they won’t be emitting any radio signals, just sitting on the ground and charging batteries with non-reflective solar cells, awaiting either a wake-up command, or a timer will activate them.
When the US decides to launch missiles, B-52 aircraft, or any other defensive measure, the Chinese will know ahead of time what’s coming, where it's coming from, and when it took off.
I’m not a military expert, but I can see how this might be used in an offensive manor, I’m sure I’m not the only person on the planet that believes this is possible, but for some reason, nobody within the US government is talking about any of this. At this point it would make sense for people in the surrounding states to look around in remote areas to see if they can spot something! Remember, we wouldn’t even have known about the first balloon if it wasn’t for regular citizens paying attention.
Note: You DO NOT need to register to leave a comment. Email addresses are NOT used. Just make one up "someone@somehost.com"
The QR code below links to WindUpRubberFinger.com for easy sharing.
Honda HVAC Mode Door Actuators
A little history first. I worked on cars for about 10 years before I went into a completely different industry. During that time I acquired all of my ASE certifications, except for Automatic Transmission. I missed the automatic transmission test by one question. 🤣 No matter, at the time I worked for Toyota, and we didn’t rebuild transmissions, we replaced them with Toyota remanufactured units, so I wasn’t worried about internal bearing clearances, I didn’t deal with that. If I needed to rebuild an automatic transmission I would refer to the manufacturer’s manual, as there are always updates to process over time anyway.
Back to actuators. In January of last year I did a post on how to repair a Honda Blend Door Actuator. This time I'm going to cover the Mode Door Actuator (the one that controls vent direction).
These actuators generally fail for the same reason the other kind do, the grease dries out and becomes stops the position feedback connections from making. The main difference is that the blend door actuators use a variable voltage feedback for position awareness. The mode door actuator uses switch contacts for position awareness.
This particular actuator is from a 2008 CR-V. The actuator is located on the passenger side to the left of the glovebox. Remove the glovebox door, the kick panel under the glovebox, and passenger side foot vent. The actuator should now be accessible.
Now I'll get into disassembling the actuator and repairing it.
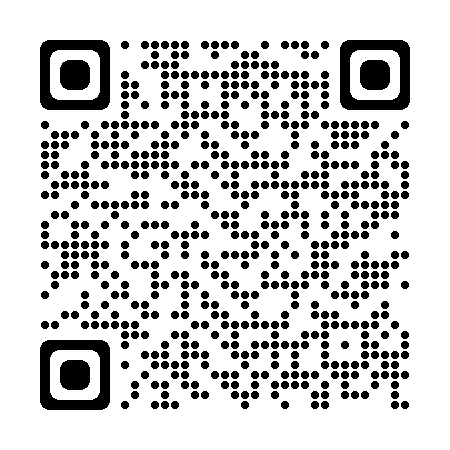
This is a view of the assembly as it looks mounted in the car. The metal bracket is between the actuator and the HVAC box.

This is a view of the output slide mechanism. This is where the door levers are manipulated.
Even before removing the bracket, I want to mark the output shaft, so that I know where it lines up. If it's clocked wrong, the actuator won't work correctly. You can see where I made a mark by scratching the plastic with a screwdriver.

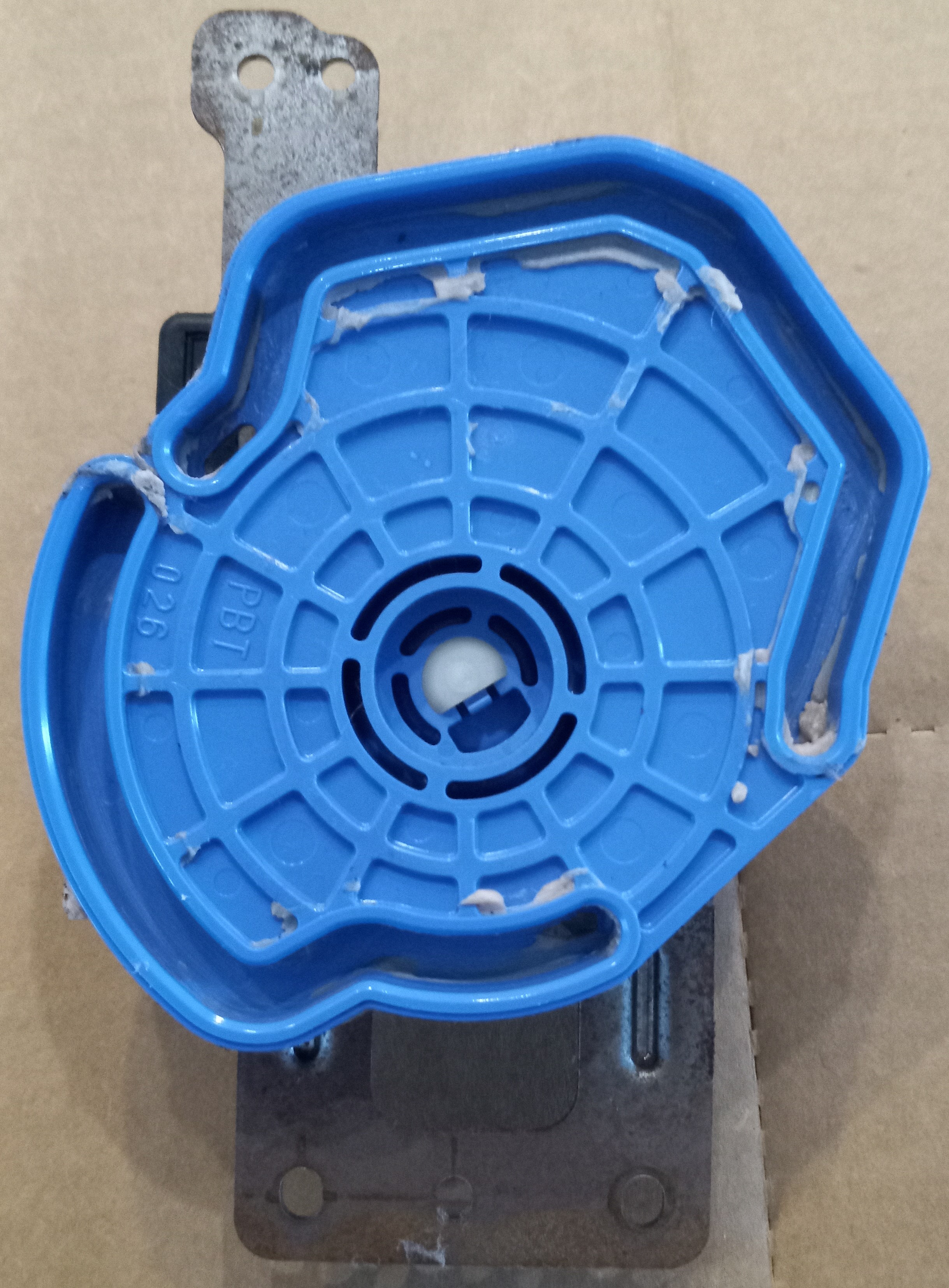
Once the bracket is removed, you have to unsnap the clips that hold the actuator housing together. They go all the way around.

In order to get all of the clips at once, I use toothpicks. I can pry the plastic just enough to get a toothpick in, then move to the next clip. Note: The clips by where plug goes almost always break off.
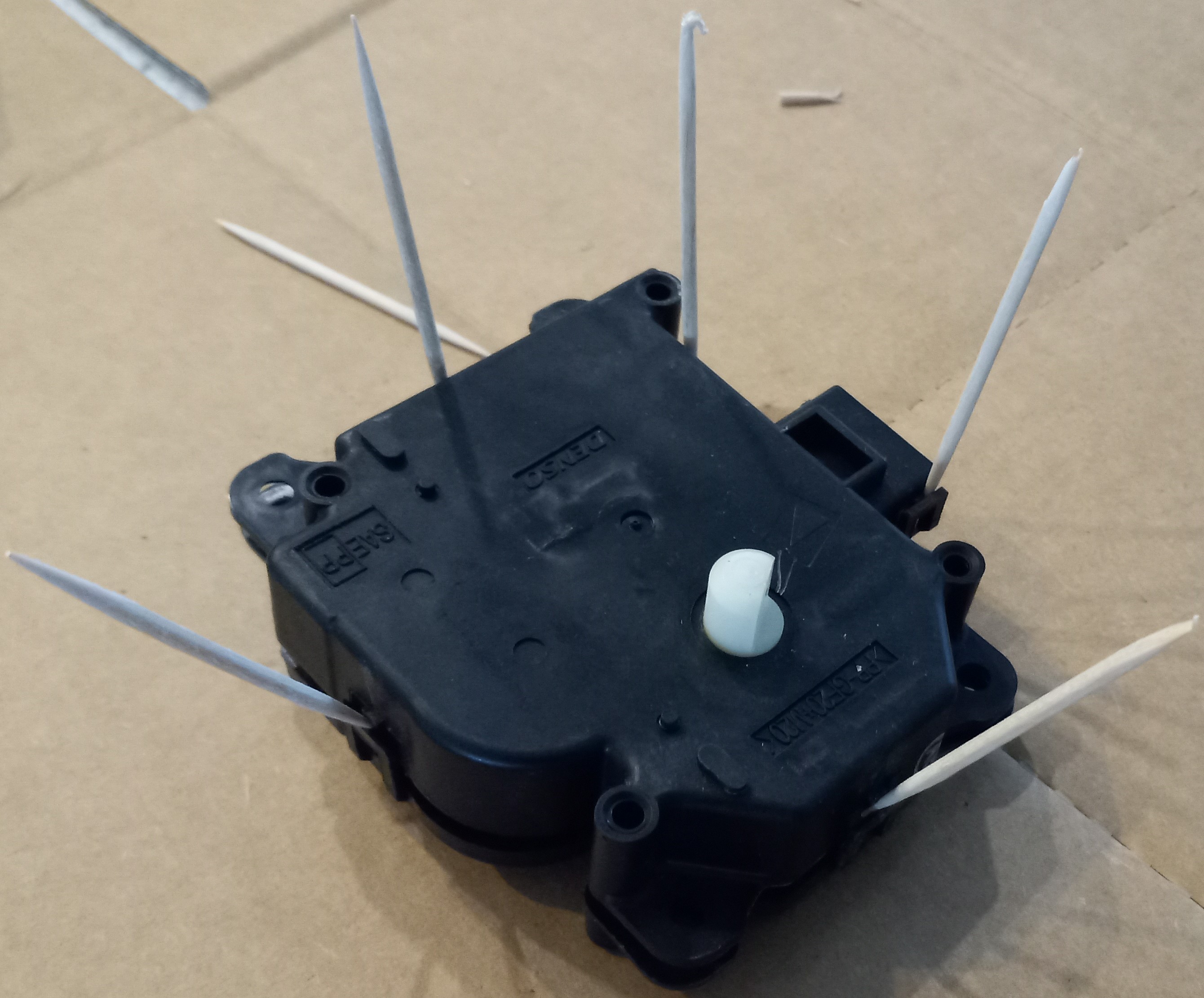
Once you have the actuator assembly open, mark the motor's position. The motor can go in either way, but it is a DC motor, so it's polarized. If you put the motor in the wrong way, the actuator will turn in the wrong direction relative to command. It won't hurt anything, but it won't work either.
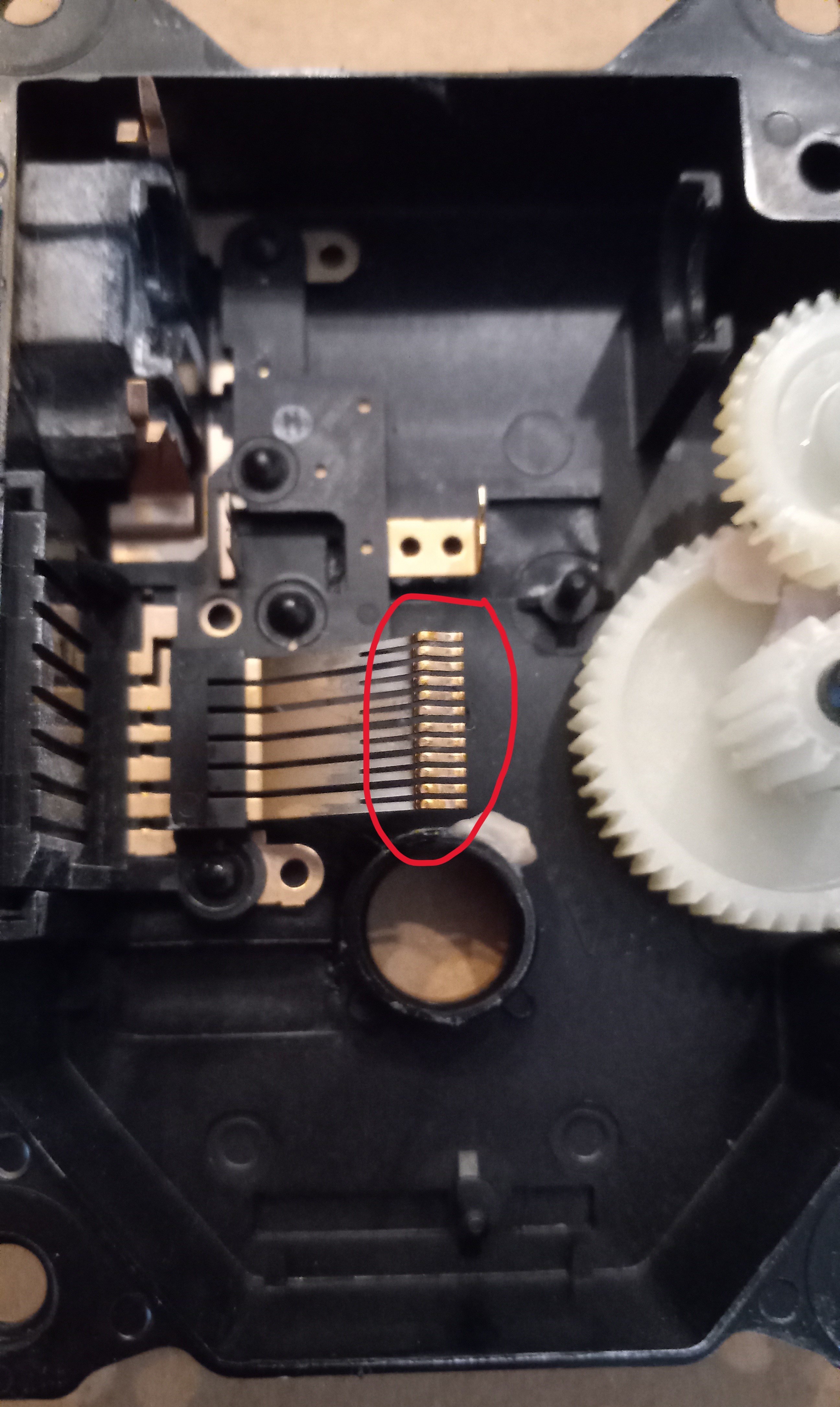
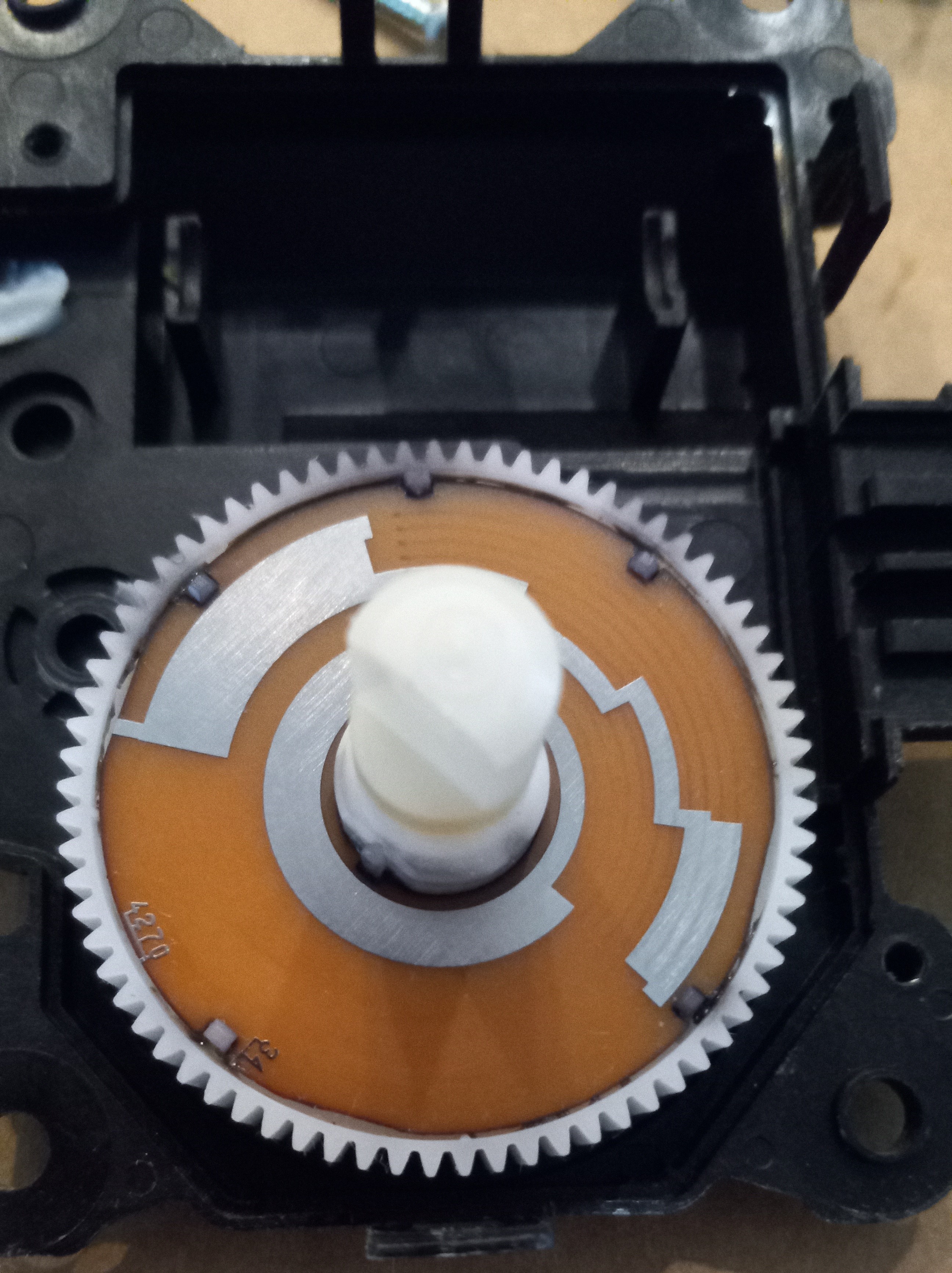
From this picture you can see the output gear. You can also see the switch contacts used to determine the position of the actuator. The old grease is thick and stopping good connection between the little copper wipers, and the positioning contacts. This is the most common issue with these actuators. Clean all of the grease off of the positioning contacts and cover with a thin coat of Vaseline.

Here you can see the little copper wipers. I also clean these off, and bend them up a little more to assure that they have good contact with the positioning contacts. Just place your finger on the plastic that secures them, and bend them up a little by hand, making sure not to bend them laterally.
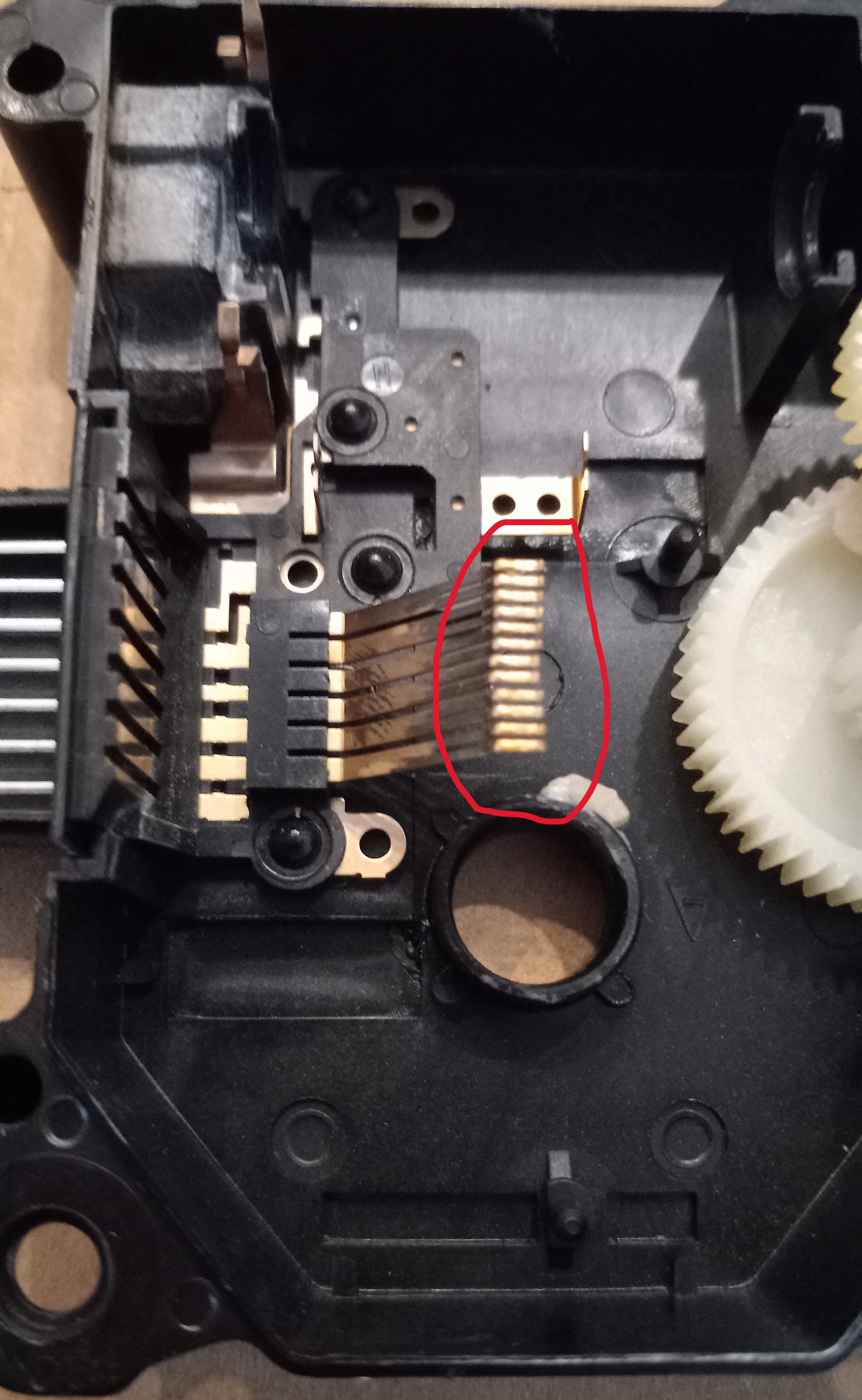
Here you can see the positioning contacts cleaned off and some Vaseline applied.
This is a closeup view of the copper wipers.
This is a view after I bent them up a little bit.

You can now reassemble the actuator making sure that the motor is in correctly, and the output shaft markings line up with where you had them. The actuator should work correctly again.
Note: You DO NOT need to register to leave a comment. Email addresses are NOT used. Just make one up "someone@somehost.com"
The QR code below links to WindUpRubberFinger.com for easy sharing.
Who is George Santos (R-NY)?
This story is interesting to me because the only reason that we're hearing about Santos lying -- is because he ran as a Republican.
Of course you could say, "Well, this guy is a politician, and all politicians lie." While this is true, it's important to realize that all people lie. The difference is what people lie about, and to whom.
However; I think that this particular incident might be a little different. I think it's possible that Santos is doing this on purpose. I know what you're thinking, "Is OGRE nuts?" I'm just wondering if this guy is doing this to prove a point. Or, should I say, I hope he's doing this to prove a point. It might be Master Level trolling. He can't be brought up on charges for lying, if that were the case nearly all of congress would be behind bars.
Former Rep. Tulsi Gabbard (D-HI) grilled embattled Rep.-elect George Santos (R-NY) about why he fabricated his resume and background, questioning whether the New York Republican “had no shame” while hosting Tucker Carlson Tonight on Tuesday.
Santos has come under fire from members on both sides of the aisle for falsifying information about his education, work history, and family history, with a string of Democratic lawmakers calling for him to step down and one of his GOP colleagues pushing for the House Ethics Committee to launch an investigation into potential violations.
“The thing is, congressman-elect, integrity means, yes, carrying yourself with honor, but it means telling the truth, being a person of integrity, and if I were one of those in New York's third district right now, now that the election is over and and finding out all of these lies that you've told, not just one little lie or one little embellishment, these are blatant lies,” the former Democratic congresswoman, who left the party earlier this year, said.
Santos has lied about the exact things that Joe Biden has lied about. That's the only reason that I think that Santos might be doing this on purpose. The media will never cover the lies that Biden has spouted over the years -- which are too many to keep track of, but they might be forced into it if Santos keeps bringing it up.
Santos attempted to pivot the conversation, alleging that President Joe Biden has “been lying to the American people for 40 years,” before Gabbard clapped back and said it was not a party issue, pressing him on his claims on the campaign trail that he was “a proud American Jew,” which he later walked back, telling the New York Post he is a practicing Catholic, but because of his family's background, identifies as “Jew-ish.”
“I've always identified as Jewish, I was raised in practicing Catholic, I think I've gone through this. Even not being raised a practicing Jew I've always joked with friends and circles, even within the campaign I say, ‘Guys, I'm Jew-ish,” he responded.
Gabbard closed out the interview alleging that Santos has not admitted “the depth of your deception” to his constituents, adding that she found it “hard to imagine how they could possibly trust your explanations.”
One thing is obvious. This guy really triggers Tulsi Gabbard! I'm just not sure why. We know he's lying, he admitted it, but that can't be the only reason that she's excessively worried about it. He mentioned Joe Biden and his lies, and Gabbard refused to go there. I found that a little odd. I know that pointing out Biden's lies would seem like beating a dead horse, but most people who weren't following politics in 1987 wouldn't know about the things Biden has lied about, or the staggering frequency. There's a large part of the voting population that has no idea about Biden being called out by the media in 1987.
Take a look:
As you can see, Biden created quite a few problems for himself in the 80s. But it's amazing how quickly people forget, or in this case, video is suppressed and hidden. This video was on YouTube for years, but was pulled when Biden was running for office.
The first part of an old news report highlights how Biden appeared to use the exact words of Neil Kinnock, a British Labour Party leader.
Comparing the speeches, it is tough to imagine that these two men had the exact same thoughts.
And since Kinnock made his speech before Biden made his, there is no way the Labour Party leader was the plagiarizer.
In fact, Biden admits to using Kinnock’s words in a later clip included in the video.
Later in King’s clip, Biden admits to plagiarizing five pages from someone else when he was in law school without accreditation.
And in the last clip of the video, the former VP claims that he went “to law school on a full academic scholarship,” “ended up in the top half my class” and was the “outstanding student” in the political science department. He also claimed to have graduated with three degrees.
The entire thing was a lie, as he later admitted he did not graduate in the top half of his class, was not named outstanding student and did not attain three degrees.
He went to school on a half scholarship, graduated near the bottom of his class (ranking 76 out of 85) and got only one degree, newscasters relate in the clip.
But that didn't stop Joe Biden did it. He's president now, and he lied about more issues than Santos. I guess it's just who you know.
Santos might be a fruitcake, or just doing what's necessary to get elected, I don't know for sure. But what's the difference really? How many "honest" politicians are elected anywhere? How many of those politicians have held true to the promises they made to the people who elected them? Isn't it just as big of a lie to make promises to voters, and never follow through?
But, some good might come of this. If Santos lies his way into office, and actually does what he says he's going to do, what then?
Note: You DO NOT need to register to leave a comment. Email addresses are NOT used. Just make one up "someone@somehost.com"
Omnibus Bill to Include Electoral Count Overhaul What Could This Mean for The Brunson Case
Schumer says he expects omnibus to include electoral count overhaul.
Speaking on the Senate floor, Schumer gave the clearest indication yet that the bill known as the Electoral Count Reform Act will be tacked on to the annual spending bill that lawmakers are rushing to finalize ahead of the holiday break.
“I expect an omnibus will contain priorities both sides want to see passed into law, including more funding for Ukraine and the Electoral Count Act, which my colleagues in the Rules Committee have done great work on,” the New York Democrat said.
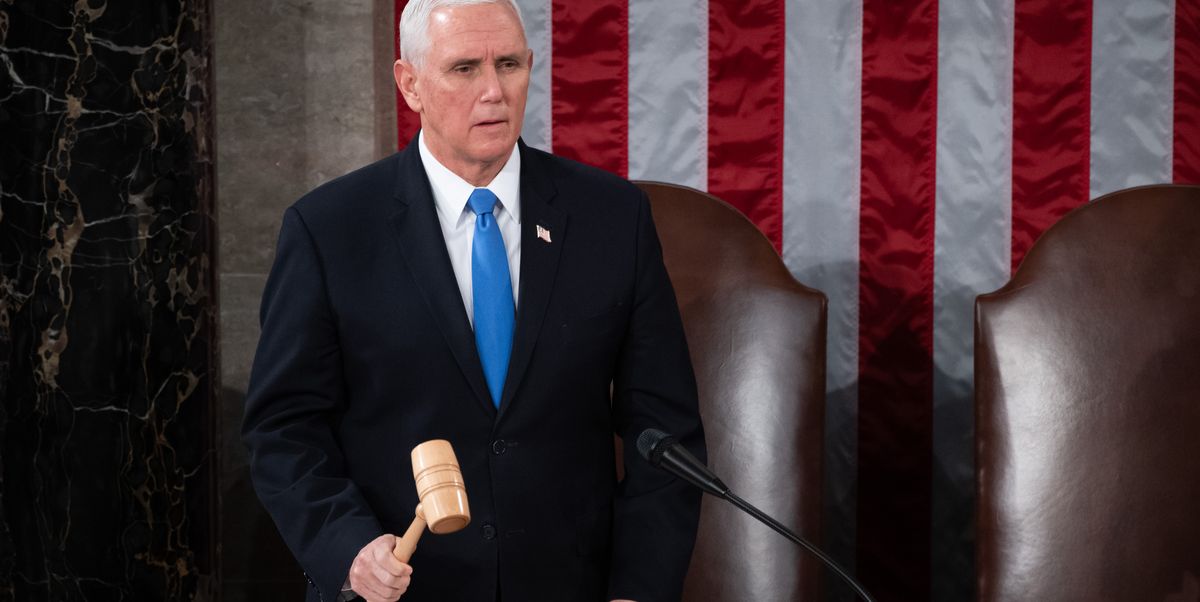
The bill is one of the most substantial legislative reactions to the ransacking of the Capitol on Jan. 6, 2021. Citing ambiguities in the Electoral Count Act of 1887, some of Trump’s backers argued that objections to the electoral vote count that day would have allowed Vice President Mike Pence to set aside some states’ results. Trump seized on those theories, urging backers to rally in Washington the morning of the count. They then stormed the Capitol.
The legislation would clarify that the vice president’s role in counting electoral votes is purely ceremonial, and that he does not have the discretion to set aside any state’s properly certified votes. It would also raise the threshold to hear objections to a state’s electors from just one member in each chamber to 20 percent of Congress.
But there is precedent for not certifying all states' results. As an example, Mark Levin said something to the effect of, "What if it was found that one state manipulated the vote to disenfranchise black voters. Would Pence still certify the election?" His point being that the vice president's job is not just to simply rubber stamp the results of every step, that's why congress gets together for the certification process to begin with. To assume otherwise is disingenuous. Not to mention this has happened before.
Supreme Court Considers Case Seeking to Overturn 2020 Presidential Election.
Supreme Court Justices may well see these approaching storm clouds and conclude that the Court’s intervention is necessary to prevent larger civil unrest resulting from constitutional violations that are undermining public trust and confidence in the outcomes of both the 2020 and 2022 elections. When criminals break the law — state and federal statutes — to rig an election, we are dependent on prosecutions by law enforcement agencies that have sadly become politicized and complicit. When they break the Constitution — the supreme law of the land — to rig an election, the only recourse may be the Supreme Court or military tribunals.
As the Brunson lawsuit argues, all of Congress was put on notice prior to its January 6th vote by more than a hundred of its own members detailing serious allegations of election frauds and calling for creation of an electoral commission to investigate the allegations.
When the results of the 1876 presidential election were in doubt, Congress created a special Electoral Commission made up of five House members, five Senators, and five Supreme Court Justices to investigate. In contrast, in early 2021 Congress had nearly two weeks to investigate before the January 20th date of the Presidential Inauguration. Had Congress waited even just one more day to January 7th, they would have received the long-awaited ODNI report reflecting a split in the Intelligence Community and the DNI’s own conclusion that the People’s Republic of China had interfered to influence the outcome of the presidential election. As Dr. Barry A. Zulauf, the Analytic Ombudsman for the Intelligence Community, concluded at the time, the Intelligence Community shamefully delayed their findings until after the January 6th Electoral College certification by Congress because of their political disagreements with the Trump administration. This paints a picture of collusion and conspiracy involving members of Congress and U.S. intelligence agencies to coverup evidence of foreign election interference and constituting the crime of High Treason.
The Brunson lawsuit does not claim the election was stolen, merely that a large majority of Congress, by failing to investigate such serious allegations of election rigging and breaches of national security, violated their Oaths to protect and defend the Constitution against all enemies, foreign and domestic – an Oath also taken by Supreme Court Justices and members of the U.S. military.
The fact that the Brunson case has made it to the Court’s docket suggests profound concerns about a lawless January 6th Congressional committee, politicized federal law enforcement and intelligence agencies, and major constitutional violations intended to overthrow an elected government by manipulating the outcome of the presidential election.
While the Brunson case is on the Court's docket, the Uni-Party is moving to make what happened in 2020, where they abdicated their duty -- the law. The question then becomes, how will the court handle the Brunson case, after congress votes to abdicates their constitutional duty? It would be a hard sell to see them hold congress accountable after they have changed the law. They would have to hold them to account for the duties they didn't perform, before the law change.
This move guarantees that future election meddling and fraud will have even fewer backstops.
-- UPDATE --
Congress passes election reform designed to ward off another Jan. 6
Lawmakers have said over and over that they want to prevent another Jan. 6-style attack on the U.S. Capitol from ever happening again.
It took almost two years, but on Friday, as part of a government spending package, Congress passed the first federal elections legislation to that aim.
The omnibus spending bill includes a section that would reform the Electoral Count Act, a 1887 law that governs the counting of Electoral College votes in Congress.
For years, legal scholars have worried the law was poorly written and in need of clarification, and former President Donald Trump and his allies targeted the law's ambiguities in their attempts to overturn the 2020 election.
In the time after voting ended in 2020 and results were certified, Trump and his team argued that then-Vice President Mike Pence had the power to interfere with the counting of electoral votes because the law as it currently stands names the vice president as the presiding officer over the joint session of Congress where those votes are counted.
They passed it, making the job of the Vice President meaningless. There was a reason it was written the way it was, and there's historical evidence that it was used in that capacity before.
Leftists don't want any more impediments to their installed candidates.
What do you think?
Please leave a comment, like it or hate it... You DO NOT need to register to leave a comment. Email addresses are NOT used. Just make one up "someone@somehost.com"