| « FDA Opens The Door To A Nationwide Healthcare Worker Shortage Via Forced Vaccinations | COVID Cases on The Rise, But Why? » |
"Informed consent disclosure to vaccine trial subjects of risk of COVID‐19 vaccines worsening clinical disease." ADE (Autoimmune Deficiency Enhancement)
ADE (Autoimmune Deficiency Enhancement) is a clear and present possibility with the current vaccines, mRNA and Viral Vector. However; the trial participants were not properly briefed on this data.
I took a full-page screenshot of the webpage from "https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7645850/" I did this specifically because I think this page will be removed once it reaches enough hits. The data within this document can be used in the court cases challenging vaccine mandates. I don't think those behind the vaccine push don't want this widely known.
Click the image to view the whole picture, then you can zoom and read it more easily.
Results of the study
COVID-19 vaccines designed to elicit neutralising antibodies may sensitise vaccine recipients to more severe disease than if they were not vaccinated. Vaccines for SARS, MERS and RSV have never been approved, and the data generated in the development and testing of these vaccines suggest a serious mechanistic concern: that vaccines designed empirically using the traditional approach (consisting of the unmodified or minimally modified coronavirus viral spike to elicit neutralising antibodies), be they composed of protein, viral vector, DNA or RNA and irrespective of delivery method, may worsen COVID-19 disease via antibody-dependent enhancement (ADE). This risk is sufficiently obscured in clinical trial protocols and consent forms for ongoing COVID-19 vaccine trials that adequate patient comprehension of this risk is unlikely to occur, obviating truly informed consent by subjects in these trials.
...
Conclusions drawn from the study and clinical implications
The specific and significant COVID-19 risk of ADE should have been and should be prominently and independently disclosed to research subjects currently in vaccine trials, as well as those being recruited for the trials and future patients after vaccine approval, in order to meet the medical ethics standard of patient comprehension for informed consent.
...
3. CONCLUSION
Given the strong evidence that ADE is a non-theoretical and compelling risk for COVID-19 vaccines and the “laundry list” nature of informed consents, disclosure of the specific risk of worsened COVID-19 disease from vaccination calls for a specific, separate, informed consent form and demonstration of patient comprehension in order to meet medical ethics standards. The informed consent process for ongoing COVID-19 vaccine trials does not appear to meet this standard. While the COVID-19 global health emergency justifies accelerated vaccine trials of candidates with known liabilities, such an acceleration is not inconsistent with additional attention paid to heightened informed consent procedures specific to COVID-19 vaccine risks.
Here is the entire text of the document:
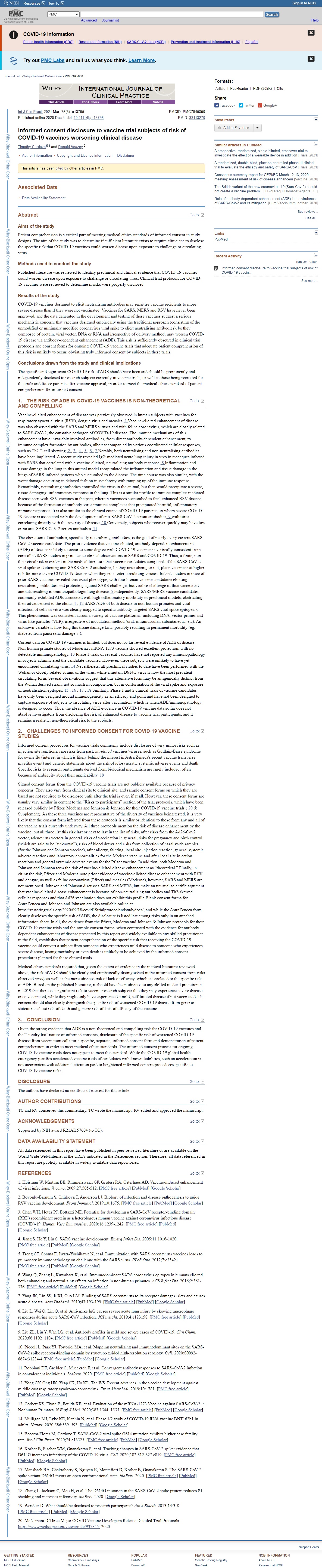
Abstract
Aims of the study
Patient comprehension is a critical part of meeting medical ethics standards of informed consent in study designs. The aim of the study was to determine if sufficient literature exists to require clinicians to disclose the specific risk that COVID-19 vaccines could worsen disease upon exposure to challenge or circulating virus.
Methods used to conduct the study
Published literature was reviewed to identify preclinical and clinical evidence that COVID-19 vaccines could worsen disease upon exposure to challenge or circulating virus. Clinical trial protocols for COVID-19 vaccines were reviewed to determine if risks were properly disclosed.
Results of the study
COVID-19 vaccines designed to elicit neutralising antibodies may sensitise vaccine recipients to more severe disease than if they were not vaccinated. Vaccines for SARS, MERS and RSV have never been approved, and the data generated in the development and testing of these vaccines suggest a serious mechanistic concern: that vaccines designed empirically using the traditional approach (consisting of the unmodified or minimally modified coronavirus viral spike to elicit neutralising antibodies), be they composed of protein, viral vector, DNA or RNA and irrespective of delivery method, may worsen COVID-19 disease via antibody-dependent enhancement (ADE). This risk is sufficiently obscured in clinical trial protocols and consent forms for ongoing COVID-19 vaccine trials that adequate patient comprehension of this risk is unlikely to occur, obviating truly informed consent by subjects in these trials.
Conclusions drawn from the study and clinical implications
The specific and significant COVID-19 risk of ADE should have been and should be prominently and independently disclosed to research subjects currently in vaccine trials, as well as those being recruited for the trials and future patients after vaccine approval, in order to meet the medical ethics standard of patient comprehension for informed consent.1. THE RISK OF ADE IN COVID-19 VACCINES IS NON-THEORETICAL AND COMPELLING
Vaccine-elicited enhancement of disease was previously observed in human subjects with vaccines for respiratory syncytial virus (RSV), dengue virus and measles. 1 Vaccine-elicited enhancement of disease was also observed with the SARS and MERS viruses and with feline coronavirus, which are closely related to SARS-CoV-2, the causative pathogen of COVID-19 disease. The immune mechanisms of this enhancement have invariably involved antibodies, from direct antibody-dependent enhancement, to immune complex formation by antibodies, albeit accompanied by various coordinated cellular responses, such as Th2 T-cell skewing. 2 , 3 , 4 , 5 , 6 , 7 Notably, both neutralising and non-neutralising antibodies have been implicated. A recent study revealed IgG-mediated acute lung injury in vivo in macaques infected with SARS that correlated with a vaccine-elicited, neutralising antibody response. 8 Inflammation and tissue damage in the lung in this animal model recapitulated the inflammation and tissue damage in the lungs of SARS-infected patients who succumbed to the disease. The time course was also similar, with the worst damage occurring in delayed fashion in synchrony with ramping up of the immune response. Remarkably, neutralising antibodies controlled the virus in the animal, but then would precipitate a severe, tissue-damaging, inflammatory response in the lung. This is a similar profile to immune complex-mediated disease seen with RSV vaccines in the past, wherein vaccinees succumbed to fatal enhanced RSV disease because of the formation of antibody-virus immune complexes that precipitated harmful, inflammatory immune responses. It is also similar to the clinical course of COVID-19 patients, in whom severe COVID-19 disease is associated with the development of anti-SARS-CoV-2 serum antibodies, 9 with titres correlating directly with the severity of disease. 10 Conversely, subjects who recover quickly may have low or no anti-SARS-CoV-2 serum antibodies.
The elicitation of antibodies, specifically neutralising antibodies, is the goal of nearly every current SARS-CoV-2 vaccine candidate. The prior evidence that vaccine-elicited, antibody-dependent enhancement (ADE) of disease is likely to occur to some degree with COVID-19 vaccines is vertically consistent from controlled SARS studies in primates to clinical observations in SARS and COVID-19. Thus, a finite, non-theoretical risk is evident in the medical literature that vaccine candidates composed of the SARS-CoV-2 viral spike and eliciting anti-SARS-CoV-2 antibodies, be they neutralising or not, place vaccinees at higher risk for more severe COVID-19 disease when they encounter circulating viruses. Indeed, studies in mice of prior SARS vaccines revealed this exact phenotype, with four human vaccine candidates eliciting neutralising antibodies and protecting against SARS challenge, but viral re-challenge of thus vaccinated animals resulting in immunopathologic lung disease. 5 Independently, SARS/MERS vaccine candidates, commonly exhibited ADE associated with high inflammatory morbidity in preclinical models, obstructing their advancement to the clinic. 4 , 12 SARS ADE of both disease in non-human primates and viral infection of cells in vitro was clearly mapped to specific antibody-targeted SARS viral spike epitopes. 6 This phenomenon was consistent across a variety of vaccine platforms, including DNA, vector primes and virus-like particles (VLP), irrespective of inoculation method (oral, intramuscular, subcutaneous, etc). An unknown variable is how long this tissue damage lasts, possibly resulting in permanent morbidity (eg, diabetes from pancreatic damage 7).
Current data on COVID-19 vaccines is limited, but does not so far reveal evidence of ADE of disease. Non-human primate studies of Moderna's mRNA-1273 vaccine showed excellent protection, with no detectable immunopathology. 13 Phase 1 trials of several vaccines have not reported any immunopathology in subjects administered the candidate vaccines. However, these subjects were unlikely to have yet encountered circulating virus. 14 Nevertheless, all preclinical studies to date have been performed with the Wuhan or closely related strains of the virus, while a mutant D614G virus is now the most prevalent circulating form. Several observations suggest that this alternative form may be antigenically distinct from the Wuhan derived strain, not so much in composition, but in conformation of the viral spike and exposure of neutralisation epitopes. 15 , 16 , 17 , 18 Similarly, Phase 1 and 2 clinical trials of vaccine candidates have only been designed around immunogenicity as an efficacy end point and have not been designed to capture exposure of subjects to circulating virus after vaccination, which is when ADE/immunopathology is designed to occur. Thus, the absence of ADE evidence in COVID-19 vaccine data so far does not absolve investigators from disclosing the risk of enhanced disease to vaccine trial participants, and it remains a realistic, non-theoretical risk to the subjects.
2. CHALLENGES TO INFORMED CONSENT FOR COVID-19 VACCINE STUDIES
Informed consent procedures for vaccine trials commonly include disclosure of very minor risks such as injection site reactions, rare risks from past, unrelated vaccines/viruses, such as Guillain-Barre syndrome for swine flu (interest in which is likely behind the interest in Astra Zeneca's recent vaccine transverse myelitis event) and generic statements about the risk of idiosyncratic systemic adverse events and death. Specific risks to research participants derived from biological mechanism are rarely included, often because of ambiguity about their applicability. 19
Signed consent forms from the COVID-19 vaccine trials are not publicly available because of privacy concerns. They also vary from clinical site to clinical site, and sample consent forms on which they are based are not required to be disclosed until after the trial is over, if at all. However, these consent forms are usually very similar in content to the “Risks to participants” section of the trial protocols, which have been released publicly by Pfizer, Moderna and Johnson & Johnson for their COVID-19 vaccine trials ( 20 & Supplement). As these three vaccines are representative of the diversity of vaccines being tested, it is very likely that the consent form inferred from these protocols is similar or identical to those from any and all of the vaccine trials currently underway. All three protocols mention the risk of disease enhancement by the vaccine, but all three list this risk last or next to last in the list of risks, after risks from the Ad26-Cov2 vector, adenovirus vectors in general, risks of vaccination in general, risks for pregnancy and birth control (which are said to be “unknown”), risks of blood draws and risks from collection of nasal swab samples (for the Johnson and Johnson vaccine), after allergy, fainting, local site injection reaction, general systemic adverse reactions and laboratory abnormalities for the Moderna vaccine and after local site injection reactions and general systemic adverse events for the Pfizer vaccine. In addition, both Moderna and Johnson and Johnson term the risk of vaccine-elicited disease enhancement as “theoretical.” Finally, in citing the risk, Pfizer and Moderna note prior evidence of vaccine-elicited disease enhancement with RSV and dengue, as well as feline coronavirus (Pfizer) and measles (Moderna), however, SARS and MERS are not mentioned. Johnson and Johnson discusses SARS and MERS, but make an unusual scientific argument that vaccine-elicited disease enhancement is because of non-neutralising antibodies and Th2-skewed cellular responses and that Ad26 vaccination does not exhibit this profile.Blank consent forms for AstraZeneca and Johnson and Johnson are also available online at https://restoringtrials.org/2020/09/18/covid19trialprotocolandstudydocs/, and while the AstraZeneca form clearly discloses the specific risk of ADE, the disclosure is listed last among risks only in an attached information sheet. In all, the evidence from the Pfizer, Moderna and Johnson & Johnson protocols for their COVID-19 vaccine trials and the sample consent forms, when contrasted with the evidence for antibody-dependent enhancement of disease presented by this report and widely available to any skilled practitioner in the field, establishes that patient comprehension of the specific risk that receiving the COVID-19 vaccine could convert a subject from someone who experiences mild disease to someone who experiences severe disease, lasting morbidity or even death is unlikely to be achieved by the informed consent procedures planned for these clinical trials.
Medical ethics standards required that, given the extent of evidence in the medical literature reviewed above, the risk of ADE should be clearly and emphatically distinguished in the informed consent from risks observed rarely as well as the more obvious risk of lack of efficacy, which is unrelated to the specific risk of ADE. Based on the published literature, it should have been obvious to any skilled medical practitioner in 2019 that there is a significant risk to vaccine research subjects that they may experience severe disease once vaccinated, while they might only have experienced a mild, self-limited disease if not vaccinated. The consent should also clearly distinguish the specific risk of worsened COVID-19 disease from generic statements about risk of death and generic risk of lack of efficacy of the vaccine.
3. CONCLUSION
Given the strong evidence that ADE is a non-theoretical and compelling risk for COVID-19 vaccines and the “laundry list” nature of informed consents, disclosure of the specific risk of worsened COVID-19 disease from vaccination calls for a specific, separate, informed consent form and demonstration of patient comprehension in order to meet medical ethics standards. The informed consent process for ongoing COVID-19 vaccine trials does not appear to meet this standard. While the COVID-19 global health emergency justifies accelerated vaccine trials of candidates with known liabilities, such an acceleration is not inconsistent with additional attention paid to heightened informed consent procedures specific to COVID-19 vaccine risks.
The trial participants were not properly warned about the dangers associated with the COVID-19 vaccines, during the vaccine trials -- meanwhile the US public was/is told that the vaccines are, "Safe and effective?"
What do you think?
Note: You DO NOT need to register to leave a comment. Email addresses are NOT used. Just make one up "someone@somehost.com"